
1.3M
Downloads
295
Episodes
A UK based Emergency Medicine podcast for anyone who works in emergency care. The St Emlyn ’s team are all passionate educators and clinicians who strive to bring you the best evidence based education. Our four pillars of learning are evidence-based medicine, clinical excellence, personal development and the philosophical overview of emergency care. We have a strong academic faculty and reputation for high quality education presented through multimedia platforms and articles. St Emlyn’s is a name given to a fictionalised emergency care system. This online clinical space is designed to allow clinical care to be discussed without compromising the safety or confidentiality of patients or clinicians.
Episodes
Wednesday May 03, 2023
Wednesday May 03, 2023
Our monthly podcast round up from St Emlyn's Blog. This month Simon and Iain discuss the prehospital use of troponin measurement in the assessment of patients with chest pain and the use of AI in medicine, as well as an update about St Emlyn's WILD.
Please do like and subscribe
Monday Apr 24, 2023
Monday Apr 24, 2023
This is the first podcast in our new series from St Emlyn's Medical School. They are specifically aimed at healthcare students and focus on the Medical Licensing Assessment (UK) presentations in particular but will be useful wherever you listen in the world.
Each episode has a standard format with a case to set the scene, a set of learning objectives, a discussion, a summary and a case resolution.
There are comprehensive listening notes on the dedicated website, as well as a growing set of other resources.
We hope you enjoy listening. The rest of the podcasts can be found on Spotify, or wherever you get your podcasts.
The music for this series (just as it is for the St Emlyn's Podcast) is composed by Greg Beardsell
Monday Apr 17, 2023
Monday Apr 17, 2023
The latest CAN is one of our brand-new 'revision editions' -- brief podcasts aimed at covering the essentials of critical appraisal for medical students and junior doctors preparing for exams.
With the help of Gregory Yates, an academic doctor based in Manchester, this episode introduces two core concepts: sensitivity and specificity. These are two ways of thinking about the accuracy of a diagnostic test. Knowing the sensitivity and specificity of an investigation will give you a decent idea of how it should be used in the emergency department.
Sensitivity (Sn) describes the chance that a test will be positive if your patient has the condition you're testing for. Some people call it the 'true positive rate' or alternatively the positivity in disease (PID) rate. If you need a hand remembering it, you can always remember that PID is a sensitive issue.
Meanwhile, specificity (Sp) considers the chance of a test being negative if the patient doesn't have the condition you're testing for. It's the 'true negative rate' or alternatively the negativity in health (NIH) rate. There are times when we particularly need a test to have a high sensitivity. This is generally when we want to be particularly confident that a test accurately identifies everyone with the relevant condition because we really don't want to miss it. We need a high sensitivity to rule out disease. (Sn-uff it out). At other times, we need to be confident that a patient with a positive test actually has the disease - for example, if the treatment is unpleasant or involves exposing patients to risk. In that case, we want a high specificity to rule in disease. (Sp-in it in).
In this CAN, we use D-Dimer as an example of a very sensitive investigation: it’s positive in nearly 100% of cases of venous thromboembolism. Specificity describes the likelihood that the test will be negative if your patient does not have the disease. We use HbA1c as an example of a highly specific investigation: it’s rarely used in the emergency department, but if it’s elevated, we can be almost certain that the patient is diabetic. HbA1c is almost never (<1%) raised in non-diabetics.
The trouble is, many patients with a positive D-Dimer do not have a venous clot, and the majority of diabetics will have a normal HbA1c! No test is perfect, and we discuss how emergency physicians weigh up sensitivity and specificity when choosing which investigations are the best "fit" for clinical decision-making. By the end of this CAN, you will be ready to do the same -- in your exams, and on the shop floor.
Monday Mar 20, 2023
Monday Mar 20, 2023
Our regular monthly round up and chat from the St Emlyn's blog. We talk about the use of artificial intelligence in research and the use of remifentanil instead of neuromuscular blockade in rapid sequence intubation. Plus more about the StEmlynsWILD conference and Simon's new role as Dean of RCEM and how you can get involved.
Monday Feb 27, 2023
Monday Feb 27, 2023
Long term listeners to the St Emlyn’s podcast may remember our series entitled ‘Critical Appraisal Nuggets’ (CANs). We are absolutely delighted to reinvigorate this project under the leadership of Professor Rick Body, with the episode on semi structured interviews.
In this easily digestible and succinct podcast Rick and Laura Howard go through the pros and cons of setting up semi structured interviews and how these can be used effectively in qualitative research.
In the latest episode, we cover a qualitative research technique: semi-structured interviews. Qualitative research might be out of your comfort zone: we’re generally more comfortable with quantitative measures – numbers and statistics. It’s something they have experience with, having previously published a paper exploring the impact of events that happen at work on the wellbeing of emergency physicians. This was a labour of love for Laura. Laura wrote a powerful blog about it here.
Semi-structured interviews are a great way to get the really rich data we need to understand something in greater depth. They allow us to ask ‘why?’ as well as just ‘what?’, ‘who?’ and ‘when?’. But reading qualitative research papers can be difficult when it takes us out of our comfort zone. In this CAN podcast, Laura and Rick take us through what semi-structured interviews are, why we might use them, how you design and conduct them, and they also have some pearls of wisdom about how to make transcribing them a lot less painful. By the end, we hope that you’ll feel confident with the basics of the technique. And if you want to practice your critical appraisal, why not put their study under the microscope?
Monday Jan 16, 2023
Monday Jan 16, 2023
A special double edition covering the blog posts from November and December and more. We discuss evidence based medicine with the DoseVF trial, and more from RECOVERY, discussion about 'what is downtime' and how we organise follow up for patients who don't live in our area and what happened at the amazing London Trauma Conference
We also announced some of the plans for StEmlynsWILD. Look out for booking details and more in the coming weeks.
Saturday Dec 10, 2022
Saturday Dec 10, 2022
Wellbeing is very complex, as it is an individual construct that is strongly aligned and interpreted through a lens of personal values, philosophy, culture, faith, and goals for life. Most importantly, wellbeing is dynamic rather than homeostatic and a subjective state determined by the individual.
Yet we use the term wellbeing to describe a wide variety of different things (often in terms of being the opposite of burnout which it most certainly isn't).
In this second episode of our series Liz Crowe discusses in detail what the literature says about wellbeing and how we may be able to use this going forward.
Please do like and subscribe. Thanks for listening.
Sunday Nov 27, 2022
Sunday Nov 27, 2022
Burnout is a term that seems to be used a lot these days, but what does it really mean? In this episode Dr Liz Crowe explains all, and will almost certainly change the way you view burnout.
Liz, who be well known to St Emyn's audiences, has just completed her PhD on "Understanding the risk and protective factors for burnout and wellbeing of staff working in the Paediatric Intensive Care Unit: PICU staff wellbeing" and has an unrivalled real world and evidence based experience of what these terms really mean.
In this first in a special series Liz goes into depth describing not only what burnout is, but how it can be measured (and the limitations of this) and most importantly how this is a system issue and not a diagnosis.
In the next episode we will discuss another commonly used term 'wellbeing'.
We think this series is incredibly important and hope you will help us share it far and wide. You can read the accompanying blogpost here.
Monday Nov 14, 2022
Monday Nov 14, 2022
In our new regular slot of the middle Monday of the month we're delighted to bring you the highlights from the St Emlyn's blog this month.,
Iain and Simon chat about batching in EDs, Ossilation in decision making and a whole lot more about trauma (chest drains, extrication, sex and TXA and rib fixation).
Please do like and subscribe and keep an eye out for our new sister website St Emlyn's Medical School and it's podcast series coming soon.
Saturday Oct 08, 2022
Saturday Oct 08, 2022
This is our round up of all that happened on the St Emlyn's blog in August 2022 (yes - we know it's a bit late, but there's been a lot going on!).
Listen to Simon and Iain discuss the latest therapies in COVID, particularly Baricitinib, calcium in trauma and how we find balance in our work-life blend.
Please do like and subscribe to the podcast and tell your friends and colleagues. We've lots of exciting stuff coming your way over the next few months.
Sunday Aug 07, 2022
Sunday Aug 07, 2022
Simon and Iain run through the latest highlights from the St Emlyn's blog and podcast, including the FORCE study, the EXIT study and more about Vitamin C in sepsis...
We hope you enjoy the podcast. Please do like and subscribe on your preferred podcast app and tell your friends and colleagues about us.
Thursday Jun 16, 2022
Thursday Jun 16, 2022
Our monthly round up of all from the St Emlyn's blog. We discuss pathways into emergency care research, pad positioning in cardioversion of AF and possible gender differences in the presciption of TXA in trauma.
We also chat about travel in Lithuania, memories of defibrillating with hand held paddles and Simon's recent forst infection with COVID.
We mention a post on Lyme disease which you can read here (especially if you live near the New Forest...)
Thursday May 12, 2022
Thursday May 12, 2022
After a brief hiatus we're back with more from the St Emlyn's Blog. We discuss a wide range of topics from crowding in Emergency Departments and the RePHILL trial to breastfeeding, genetic testing and diagnosing DVTs, as well as our highlights from the recent RCEM CPD Conference in Bournemouth. There really is something for everyone!
Thursday Jun 17, 2021
Thursday Jun 17, 2021
It's been a busy month on the blog with plenty for Iain and Simon to talk about. The Manchester Arena bombing, new guidelines for Anaphylaxis management, Adult Congenital Heart Disease, Calcium in Major Haemorrhage and Spontaneous Coronary Artery Dissection all get a mention alongside the usual witterings of two middle aged emergency physicians.
Wednesday May 26, 2021
Wednesday May 26, 2021
This is the second in a two part podcast series discussing Adult Congenital Heart Disease (ACHD) and how these patients may present to the Emergency Department (ED). Dr Sam Fitzsimmons, our guest on the podcast, is a Consultant in Adult Congenital Heart Disease at University Hospital Southampton. There is more information in this blog post.
In this episode we discuss Eisenmenger Syndrome, Transposition of the Great Arteries and Coarctation of the Aorta.
Thursday May 20, 2021
Thursday May 20, 2021
This is the first in a two part podcast series discussing Adult Congenital Heart Disease (ACHD) and how these patients may present to the Emergency Department (ED). Dr Sam Fitzsimmons, our guest on the podcast, is a Consultant in Adult Congenital Heart Disease at University Hospital Southampton. There is more information in this blog post.
Look out for Part 2, which will be released next week, where we discuss Eisenmenger Syndrome, Transposition of the Great Arteries and Coarctation of the Aorta.
Background
With advances in paediatric cardiac surgery, more and more patients with complex congenital heart disease are surviving to adulthood: in the 1950s you might expect a survival rate of about 10%, whereas now this is more like 85%. In fact, there are more patients in the adult congenital heart disease population than there are in the paediatric one (with 2.3 million adults vs 1.9 million children in Europe).
Many patients with Adult Congenital Heart Disease are young and able to live a relatively normal life. This means that they can travel and take part in just the same sort of activities as those without ACHD. They may well turn up in your Emergency Department one day, regardless of whether you are a tertiary centre or a district general hospital (DGH).
They are experts, and know their disease well, but this does not abstain you from a responsibility to know about them too! When these patients become unwell, they can go downhill very fast and you may not have the chance to discuss with them their exact lesion and its management.
The anatomy and physiology of these patients is abnormal, so they may present in atypical ways, and may not respond to usual medical interventions: in fact, some of our usual treatments may even be harmful.
However, starting with our usual 'ABC' approach is by far the best way to go, whilst gathering more information and contacting their specialist centre. Many patients will have their last clinic letter and ECG with them (which will also have the direct dial number of their specialist). And if they, or their relative, say there is something wrong you must believe them and do all you can to make sure they are fully investigated.
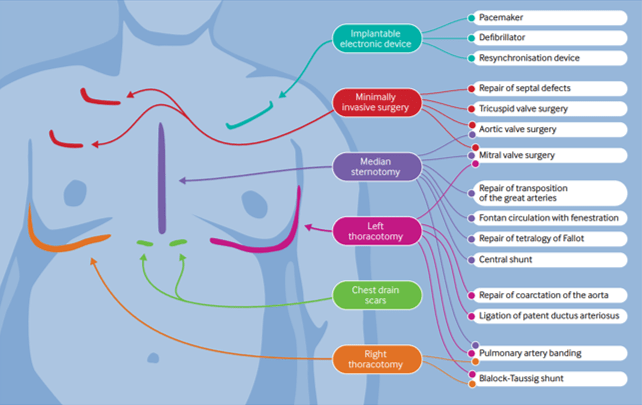
The presence of scars may give you some clues as to the patient's underlying condition and previous surgical repairs. (BMJ 2016; 354: i3905)
A General Approach
- Do your usual ABC assessment.
- Pay particular attention to the respiratory rate - this should be normal.
- Give oxygen if they look unwell.
- They should have a 'normal' blood pressure - any hypotension should be taken as abnormal and investigated.
The Fontan Circulation
This is not a condition in itself, but in fact the resulting circulation after a series of operations that could've been performed due to a number of different underlying conditions:
- Tricuspid Atresia
- Double Inlet Left Ventricle
- Atrio-ventricular Septal Defect – unbalanced
- Pulmonary Atresia
- Hypoplastic Left Heart Syndrome
In essence these patients are born with a single functioning ventricle, that has to be utilised to supply the systemic side of the circulation, whilst the Fontan acts as a passive means of returning blood to the pulmonary circulation.
It was first devised in the early 1970s by Dr Francis Fontan, so the majority of patients with this are in their mid thirties and younger.
Potential reasons for admission to the ED - Fontan circulation
1, Arrythmia
As the patient is entirely dependent on their systemic ventricle to work optimally, any disturbance of the delivery into it is very poorly tolerated. Thus, any arrhythmia is life threatening, even a mild atrial tachycardia.
These patients need to be returned to sinus rhythm as quickly as possible and the recommended method for this is DC cardioversion in expert hands.
Fontan patients have an incredibly fragile circulation and any change in their respiratory physiology can be life threatening, especially if it increases their pulmonary pressures (and thus prevents the passive flow within the Fontan circulation). These patients are not candidates for sedation in the ED and should have an experienced anaesthetist to manage them during the procedure.
Beware if the patient comes in and tells you they are fasted! This means they have been in this situation before and needed DC cardioversion.
2, Haemoptysis
Over time the patient develops venous hypertension within the Fontan connection. This causes the formation of collateral vessels, that may link into the bronchial arterial tree.
If the patient presents in shock treat them as you would any other patient with emergency blood transfusion.
Any haemoptysis, however small, may herald the beginning of a massive bleed. These patients need further investigation, probably a CT chest with contrast. These vessels may then be coiled by interventional radiology.
3, Cyanosis
If the patient has a non fenestrated Fontan they should have normal oxygen saturations. However, if there is a fenestration there will be shunting and therefore a reduction in oxygenation.
For patients this is trade of between being pink or blue, each of which have complications.
Dr Sam Fitzsimmons
Dr Sam Fitzsimmons is a Consultant Cardiologist in Adult Congenital Heart Disease (ACHD) at the University Hospital Southampton, UK. Sam also subspecialises in pulmonary hypertension and maternal cardiology. Working within a tertiary surgical ACHD centre, Sam delivers an ACHD on call service for emergency admissions, inpatient care, routine outpatient follow-up, intra-operative imaging and post-surgical care, as well as specialist clinics in Pulmonary Hypertension and Maternal Cardiology. Sam holds a Honorary Senior Clinical Lecturer post with the University of Southampton as she is passionate about teaching and in particular, she is enthusiastic about helping demystify congenital heart disease for many non-specialist to improve patient care. Sam is well published in peer review journals, cardiology textbooks and specialist guidelines.
Friday May 14, 2021
Friday May 14, 2021
A podcast with Iain and Simon summarising all the latest content from the St Emlyn's blog in April 2021. Topics discussed include Vaccine Induced Thrombocytopenic Thrombosis, how our own biases can effect our critical appraisal and whether we need to worry about grading the quality of FOAMed resources.
Thanks for listening. Please check out the blogs themselevs at www.stemlynsblog.org and consider subscribing and rating us on iTunes.
If you'd like to see some more from Peter Brindley you can watch one of his SMACC talks here.
Monday Mar 15, 2021
Monday Mar 15, 2021
Our regular podcast round up from February 2021. Iain and Simon highlight the key learning points from this month on the St Emlyn’s blog and podcast.
Topics discussed this month include tocilizumab in COVID19, TIA risk scores, new Emergency Care standards (targets) and TXA use in epistaxis. We also pay tribute to Dr Cliff Mann, former President of RCEM who sadly died this month.
Please remember to subscribe to the podcast on iTunes/Google Play and please do leave us some reviews and ratings there.
Sunday Jan 17, 2021
Sunday Jan 17, 2021
A vaccine update with Rick Body, Simon Carley, Pam Vallely, Paul Klapper and Charlie Reynard. Bringing RCEM, St Emlyn's and the University of Manchester together for the latest thoughts and wisdom on the vaccines that might get us out of this pandemic.
Moderna vaccine phase 3 trial - https://www.nejm.org/doi/full/10.1056/nejmoa2022483
Oxford vaccine phase 2/3 - https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(20)32466-1.pdf
Pfizer vaccine trial - https://www.nejm.org/doi/full/10.1056/NEJMoa2034577
#vaccines #COVID19 #coronavirus
Thursday Dec 17, 2020
Thursday Dec 17, 2020
A special festive edition of our round up podcast featuring six weeks of blog posts and plenty more besides.
From all at St Emlyn's we hope you have a very happy festive season and we cannot wait to talk to you again in 2021.
Take care,
Simon and all the team
Friday Nov 06, 2020
Friday Nov 06, 2020
A bumper edition of the podcast where Iain and Simon discuss TXA (twice), antibiotics in appendicits, VTE, Blood products in trauma, use of ultrasound in cardiac arrest and plasma in traumatic brain injury. Oh, and COVID19 (but not for long)...
An evidence based cornucopia of aural pleasure.
Please like and subscribe (as all podcasters seem to say).
Take care,
Iain
Saturday Oct 24, 2020
Saturday Oct 24, 2020
In this special edition of the podcast, Liz Crowe discusses with Iain how we can find contentment, despite the relentless nature of COVID19 and the impending second wave. She gives practical, realistic advice that everyone can consider and encourages us all to be kind to ourselves in these strange and difficult times.
Wednesday Sep 23, 2020
Thursday Sep 10, 2020
Thursday Sep 10, 2020
Welcome to our audio round up of everything on the blog during August.
As the world continues to be in the grips of the Coronavirus pandemic there have been more papers looking at all aspects of this disease.
Simon reviewed the latest paper on Hydroxychloroquine and Charlie collated some of the top papers covering aspects from aerosol spread and use of CPAP to the effect on vulnerable groups and the effect on staff psychological health
It's not all COVID though. Sepsis is a condition we all want to be able to treat more effectively. Sadly there doesn't seem to be any encouraging news about the use of Vitamin C, Steroids and Thiamine in this latest RCT.
Many of the St Emlyn's group have special expertise in toxicology and Gareth wrote this incredibly informative post about the use of GBL. If you're not sure what "ChemSex" is then this post from a few years ago by Janos is worth a read.
The anonymously written "Look at what they make you give" post really struck a chord with readers, with an astonishing number of views. There are messages here for us all.
The numbers of Lesson Plans available continue to grow. We've had some great feedback following their use in induction. If tyou've not seen them yet, do have a look and let us know what you think.
Saturday Aug 01, 2020
Saturday Aug 01, 2020
Our own version of Buy One Get One Free* this month, where you get a round up of two months of blog content.
Coronavirus continues to dominate the medical (and non-medical) headlines, and we discuss the two major results from the RECOVERY trial published recently, one positive and one not so (depending on who you talk to....). Simon also catches up with Roberto Cosentini, who you'll remember from the very powerful podcast at the beginning of the pandemic.
COVID isn't the only EBM circus in town though: we've reviewed HALT-IT and Simon has given a talk about the "Ten Top Trauma Papers" of the last year and Laura reviewed a paper looking at haloperidol for headaches.
We're having to think even harder about how we communicate in the ED, both for clinical care and to deliver education. Two ideas to help learning have been featured this month: The St Emlyn's Lesson Plans and "Background Learning".
Good luck to all those starting in Emergency Medicine, and a huge thank you to all those who are moving to other areas of medicine or other departments. It's been a curious few months...
Take care,
Iain
*It's actually Get One Free Get Another Free, but whose ever heard of that?
Thursday Jun 25, 2020
Thursday Jun 25, 2020
We are delighted to introduce you to the "St Emlyn's Lesson Plans", which we hope will help structure some of your education sessions over coming months (and years).
Each lesson plan starts with a descrete learning outcome, to set the scene, as well as details of the RCEM curriculum item(s) that will be covered.
The first tasks are aimed at aquiring some background knowledge and can either be done as part of the session, or beforehand. These utilise the vast "FOAMed" resources (including, but not exclusively, those of St Emlyn's).
Our experience is that time constraints often mean that "background reading" isn't achieved before the session, so would encourage allowing time within it to complete these. They are designed to take about 30 minutes and occupy the first half of the session.
Everything you need for each lesson is included in the plan. We would recommend that each learner has an internet enabled device available (with headphones) to read and listen to the background material at their own pace.
The second half of the session should be facilitated by an expert. This can happen in person, but also online, via any of the interfaces that are now so familiar.
In many plans we have given some case examples, but it would be even better if learners can bring cases of their own for discussion. This element is very much within the control of the facilitator (who should been fully cogniscent of the contents of the knowledge section).
The session finishes off with a summary, this should emphasise again the most important learning points. To really embed the knowledge and skills the particiapants should be encouraged to reflect on what they have learned, and to even talk to thse who were unable to attend about what they missed.
For learners this also gives an opportunity to easily link teaching sessions to their portfolio.
You may want to record the "face-to-face" elements, so that those who were not present are able to access them when they can (and those that did can rewatch to refresh their learning).
Although these plans are designed for delivery in a single centre, there is absolutely no reason why regional (or even national) teaching could take place in this way. The recent COVID19 Journal Clubs have demonstrated beautifully how a group of learners can engage with an online panel.
We would be very happy to receive lessons plans to add to the collection. This is very much a collaborative effort.
Please let us know what you think of these lesson plans and if you are using them in your Department. We'd love to hear your ideas about how we can take medical education forward.
Friday Jun 19, 2020
Friday Jun 19, 2020
St Emlyn's three professors, Carley, Body and Horner* critically appraise the Press Release regarding Dexamethasone in the treatment of COVID-19.
What does this mean for the future of Evidence Based Medicine? Can we really start using a medication when the trial hasn't been peer reviewed and the full dataset not released?
The blog post by Josh Farkas, that is mentioned in the podcast, is here.
*Professor Simon Carley, Professor of Emergency Medicine at Manchester Metropolitan University and a Consultant in Adult and Paediatric Emergency Medicine at Manchester Foundation Trust, Professor Rick Body Professor of Emergency Medicine in Manchester and Honorary Consultant in Emergency Medicine at Manchester Foundation Trust. Professor Dan Horner, Professor of Emergency Medicine of the Royal College of Emergency Medicine and Consultant in Emergency Medicine and Intensive Care at Salford Royal NHS Foundation Trust.
Thursday Jun 04, 2020
Thursday Jun 04, 2020
Welcome to our seventh webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn's.
The live event took place on Tuesday 26th May.
Today's panel will be hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar, Prof Pam Vallely (Professor of Medical Virology), Ellie Hothershall (Consultant in Public Health), Prof Simon Carley and special guest Kelly Ann Janssens (Emergency Physician in Ireland) to discuss five papers about COVID-19 infection.
This will be the last weekly journal club, but we will be back with more EBM goodness very soon. Do let us know what you like to be included at stemlyns@gmail.com
References
-
Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 — Preliminary Report. N Engl J Med. Published online May 22, 2020. doi:10.1056/nejmoa2007764
-
Mehra MR, Desai SS, Ruschitzka F, Patel AN. Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis. The Lancet. Published online May 2020. doi:10.1016/s0140-6736(20)31180-6
-
Gray N, Calleja D, Wimbush A, et al. “No test is better than a bad test”: Impact of diagnostic uncertainty in mass testing on the spread of Covid-19. Published online April 22, 2020. doi:10.1101/2020.04.16.20067884
-
Peyrony O, Marbeuf-Gueye C, Truong V, et al. Accuracy of Emergency Department clinical findings for diagnostic of coronavirus disease-2019. Annals of Emergency Medicine. Published online May 2020. doi:10.1016/j.annemergmed.2020.05.022
-
Ludvigsson JF. Children are unlikely to be the main drivers of the COVID‐19 pandemic – a systematic review. Acta Paediatr. Published online May 19, 2020. doi:10.1111/apa.15371
Friday May 22, 2020
Friday May 22, 2020
Welcome to our sixth COVID-19 Journal Club Podcast.
The panel was hosted by Rick Body and included Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar, Prof Pam Vallely (Professor of Medical Virology), Prof Simon Carley and special guest Liz Crowe (Advanced Clinician Social Worker and PhD candidate in health staff wellbeing in Brisbane) to discuss four papers about COVID-19 infection. We were especially pleased to welcome Liz this week, which enabled us to focus on the important topics of grief, loss and communication during the COVID-19 pandemic.
References
Friday May 15, 2020
Friday May 15, 2020
Welcome to our fifth webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn’s.
The live event took place on Tuesday 12th May at 11.00am BST (10.00am GMT).
The COVID-19 Journal Club Panel
Today’s panel was hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Prof Dan Horner, Dr Anisa Jafar, Prof Pam Vallely (Professor of Medical Virology), Prof Simon Carley and special guest Lauren Westafer (Attending in Emergency Medicine and Co-Creator of the Foamcast blog and podcast) and Ellie Hothershall (head of undergraduate medicine at the University of Dundee and an expert in Public Health) to discuss six papers about COVID-19 infection.
Wednesday May 13, 2020
Wednesday May 13, 2020
Over the last few years many of us in the UK have started to incorporate high-sensitivity troponin into the assessment of patients presenting with chest pain.
We have seen these samples taken at ever shorter intervals, aiming to discharge low risk patients safely, sooner from the Emergency Department (ED). This has been driven in part by the "Four Hour Emergency Access Target" as well as increased crowding in overwhelmed EDs.
In this podcast, internationally renowned researcher Prof Rick Body discusses the latest in troponin research and the recent LoDED study.
The Shownotes
The various organisations mentioned by Rick can be found here:
The Innovation Agency Webinar Series
The NHS Accelerated Access Collaborative
The CQUIN that will be implemented later this year (page 15 for the Troponin section)
The Draft NICE recommendations
Thursday May 07, 2020
Thursday May 07, 2020
Welcome to our fourth webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn's.
The live event tool place on Tuesday 5th May at 11.30am BST (10.30am GMT).
The panel was again be hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar (Academic Clinical Lecturer), Prof Pam Vallely (Professor of Medical Virology), Prof Simon Carley and special guest Justin Morgenstern to discuss six papers about COVID-19 infection.
There will be another COVID 19 Journal Club next week (Tuesday 12th May at 11am).
References
Podcast edited from a live webinar by Izzy Carley
Sunday May 03, 2020
Sunday May 03, 2020
It's been another busy month at St Emlyn's, with the publication of 15 blog posts and five podcasts, but there does seem to be an awful lot to talk about!
Of course there have been multiple posts and podcasts about COVID-19, and you can fiind all of these on our special St Emlyn's page. Highlights have included the three RCEM/St Emlyn's Webinars which we are delighted to host in podcast form.
It's not just been coronavirus though, we have also dipped out toes into exercise and nutrition, graphic design and horticulture!
Parts of the site have also undergone a bit of a redesign with the curriculum pages now easier to navigate to find that post to fioll an e-portfolio hole.
We hope you're finding all of our output useful. Please do subscribe to the website (in the top right hand corner) and rate our podcast on iTunes.
They'll be much more to come in May I am sure.
Take care
Iain
Podcast edited by Izzy Carley
Thursday Apr 30, 2020
Thursday Apr 30, 2020
Welcome to our third webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn’s.
The live event took place on Tuesday 28th April at 11am BST (10am GMT).
The panel was hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Dan Horner (RCEM Professor), Prof Pam Vallely (Professor of Medical Virology), Salim Rezaie (Emergency Physician and Founder of REBEL EM) and Prof Simon Carley (you know him…) to discuss five papers about COVID-19 infection. There will be another COVID 19 Journal Club next week (Tuesday 5th May at 11am).
Edited by Izzy Carley and Iain Beardsell
References
-
Helms J. High risk of thrombosis in patients in severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Medicine. April 2020:1-21. https://www.esicm.org/wp-content/uploads/2020/04/863_author_proof.pdf.
-
Caputo ND, Strayer RJ, Levitan R. Early Self‐Proning in Awake, Non‐intubated Patients in the Emergency Department: A Single ED’s Experience during the COVID‐19 Pandemic. Acad Emerg Med. April 2020. doi:10.1111/acem.13994
-
Garcia FP, Perez Tanoira R, Romanyk Cabrera JP, Arroyo Serrano T, Gomez Herruz P, Cuadros Gonzalez J. Rapid diagnosis of SARS-CoV-2 infection by detecting IgG and IgM antibodies with an immunochromatographic device: a prospective single-center study. April 2020. doi:10.1101/2020.04.11.20062158
-
Richardson S, Hirsch JS, Narasimhan M, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. April 2020. doi:10.1001/jama.2020.6775
-
Metzler B, Siostrzonek P, Binder R, Bauer A, Reinstadler S. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: the pandemic response causes cardiac collateral damage. Eur Heart J. April 2020. doi:10.1093/eurheartj/ehaa314
Saturday Apr 25, 2020
Saturday Apr 25, 2020
Welcome to our second webinar on recent research about COVID-19, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn’s.
The panel was hosted by Rick Body. The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Prof Pam Vallely (Professor of Medical Virology), Dr Anisa Jafar (Academic Clinical Lecturer), Dr Casey Parker and Prof Simon Carley (you know him…) to discuss six papers about COVID-19 infection.
The live event took place on Tuesday 21st April 2020
References:
Paper 1 (00:00) Tang W, Cao Z, Han M, et al. Hydroxychloroquine in patients with COVID-19: an open-label, randomized, controlled trial. April 2020. doi:10.1101/2020.04.10.20060558
Wednesday Apr 15, 2020
Wednesday Apr 15, 2020
Professor Rick Body is joined by Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynolds (NIHR Clinical Research Fellow), Prof Pam Vallely (Professor of Medical Virology), Dr Anisa Jafar (Academic Clinical Lecturer) and Prof Simon Carley (you know him...) to discuss six papers about COVID-19 infection.
03:10 - Paper 1 – Guan et al. Clinical characteristics of Coronavirus disease 2019 in China. NEJM Feb 28 2020
https://www.nejm.org/doi/full/10.1056/NEJMoa2002032
16:54 Paper 2 – Zou et al. Single Cell RNA-SEQ Data Analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-NCOV infection. Frontiers of Medicine. Mar 12 2020.
https://link.springer.com/content/pdf/10.1007/s11684-020-0754-0.pdf
21:43 Paper 3 – Gautret et al. Hydroxychloroquine and azithromycin treatment of COVID-19: Results of an open-label non-randomised clinical trial. International Journal of Antimicrobial Agents. 20 Mar 2020
https://www.sciencedirect.com/science/article/pii/S0924857920300996?via%3Dihub
25:25 Paper 4 – Cao et al. A trial of Lopinavir-Ritonavir in adults hospitalized with severe COVID-19. NEJM Mar 18 2020
https://www.nejm.org/doi/pdf/10.1056/NEJMoa2001282
29:35 Paper 5 – Cui et al. Prevalence of venous thromboembolism in patients with severe Coronavirus pneumonia. Journal of Thrombosis and Haemostasis. Apr 9 2020 doi:10.1111/jth.14830
https://onlinelibrary.wiley.com/doi/epdf/10.1111/jth.14830
34:14 Paper 6 – Lynarts et al. Prediction models for diagnosis and prognosis of COVID-19 infection: systematic review and critical appraisal. BMJ. Apr 7 2020 BMJ 2020;369:m1328
Sunday Apr 05, 2020
Sunday Apr 05, 2020
Iain and Simon discuss Covid19 and more in this review of the best of the blog from March 2020.
Thursday Apr 02, 2020
Thursday Apr 02, 2020
Simon interviews Dr John Rogers and Dr Nathan Lewis on respiratory infection prevention.
John a Sports and Exercise Medicine Consultant in Manchester. He is also Chief Medical Officer for British Triathlon and Visiting Professor in Sport & Exercise Medicine at Manchester Metropolitan University.
Nathan is lead performance nutrition scientist at the English Institute of Sport and at ORRECO.
These two academics take us through how sports science might be able to support our wellbeing during the Covid19 pandemic.
References
- Recommendations to maintain immune health in athletes https://www.tandfonline.com/loi/tejs20
- Probiotics https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006895.pub3/epdf/full
- Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials https://pubmed.ncbi.nlm.nih.gov/23840373/
- Vitamin C for prevention and treatment of pneumonia https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013134/full
- Vitamin C and common cold https://www.cochrane.org/CD000980/ARI_vitamin-c-for-preventing-and-treating-the-common-cold
- Effect of Flavonoids on Upper Respiratory Tract Infections and Immune Function: A Systematic Review and Meta-Analysis https://pubmed.ncbi.nlm.nih.gov/27184276/
- Vitamin C and Infections https://pubmed.ncbi.nlm.nih.gov/28353648/
- Zinc lozenges and the common cold: a meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage https://pubmed.ncbi.nlm.nih.gov/28515951/
Sunday Mar 29, 2020
Sunday Mar 29, 2020
The world is consumed by the Coronavirus pandemic, but how do we look after ourselves? Liz and Iain discuss some strategies to stay well over the coming weeks and months. Recorded on 25th March 2020.
Tuesday Mar 24, 2020
Tuesday Mar 24, 2020
Simon chats to Sarah Thornton, consultant anaesthetist, intensivist and head of the NW school of anaesthesia on preparing to work in a critical care unit during the Covid-19 pandemic.
Friday Mar 20, 2020
Friday Mar 20, 2020
Iain and Simon chat about the current Corona pandemic and the blog in Feb 2020.
Iain remains positive, but Simon thinks the glass is half full. Time will tell who is right (though in truth there is a lot of common ground).
S
Saturday Mar 14, 2020
Saturday Mar 14, 2020
Dr Roberto Cosentini is an old friend of St Emlyn's who works in Bergamo, in Northern Italy. He is right at the heart of the recent Covid19 outbreak. He kindly found an hour to record a podcast with us on his experiences.
There are so many essential lessons in this podcast. Please share with clinical and non-clinical colleagues, as we need to plan NOW. Roberto is quite clear that if we don't train and get plans into place before the wave of cases hit us then both ourselves and our patients will suffer.
In the interest of speed I'm not going to summarise the whole podcast. You have to listen to it all yourself to see what's relevant to you. These are some of my take away messages.
- Divide your department into resp patients and non-resp patients
- Wear PPE and know how to use it
- You will need clinicians who do not usually work in ED. Train and orientate them now (before you need them).
- Most patients are hypoxic and this responds to O2 and CPAP. You're going to need a lot of CPAP and how that happens could be tricky. They found hoods the best (Ed - but how many of those do we have?).
- Although hypoxic, patients have good lung compliance.
- They regularly saw diurnal variation with many patients presenting in the early afternoon.
- It's emotionally exhausting. Prepare yourself and your team psychologically and support them during the pandemic. Roberto's department has an embedded psychologist.
- Health care worker infections were quite low (because they wore PPE for all resp cases).
- Flow through the department and onto wards is absolutely vital.
- Flow out the the main hospitals to other units that can rehabilitate is vital.
- Decisions for ICU level care were similar to normal (in his hospital)
We rarely declare one of our podcasts a 'must listen' but this is an exception. Please listen and share widely. Please think hard about the issues Roberto raises and PLEASE ACT NOW.
vb
S
How you can support St Emlyn's
- Join us for #stemlynsLIVE conference May 12th 2020
- Subscribe to the blog (look top right for the link)
- Subscribe to our PODCAST on iTunes
- Follow us on twitter @stemlyns
- PLEASE Like us on Facebook
- Find out more about the St.Emlyn’s team
- Find out more about the MMU MSc in Emergency Medicine here.
- Download one of our FREE e-books here

Wednesday Feb 12, 2020
Wednesday Feb 12, 2020
Iain is back on the podcast with Simon to talk through the best of the blog from January 2020.
Monday Dec 23, 2019
Saturday Dec 07, 2019
Saturday Nov 02, 2019
Saturday Nov 02, 2019
A Month in Review: Key Takeaways from St Emlyn's September 2019 Content
Welcome to a detailed overview of the latest content from St Emlyn's, focusing on the valuable insights and educational resources we shared throughout September 2019. This month’s offerings span a wide range of topics, from the evolving concept of the "resuscitationist" to the increasing challenges posed by decompensated liver disease, and the ongoing development of emergency medicine education. Here’s a look at the most important takeaways.
The Resuscitationist: More Than Just a Title
The term "resuscitationist" has become a buzzword within the emergency medicine (EM) and critical care communities, especially following its emergence from the SMACC (Social Media and Critical Care) conferences. Dan Horner delved into this concept in a recent presentation, sparking a broader discussion about what it truly means to identify as a resuscitationist.
At its core, being a resuscitationist isn’t just about having an interest in the resuscitation room. It requires a blend of sharp clinical skills, deep knowledge of resuscitation science, and the ability to apply evidence-based practices effectively. But beyond technical expertise, leadership and teamwork are crucial. A resuscitationist must excel in managing high-stakes, chaotic situations where decisions are made with limited information and under intense time pressure.
Moreover, Dan highlights the importance of humility and collaboration. The best resuscitationists are those who recognize their own limitations and are skilled at drawing on the strengths of others, whether from different specialties or professions. This collaborative approach not only enhances patient care but also builds stronger, more effective resuscitation teams.
Decompensated Liver Disease: A Growing Concern in the ED
Liver disease is on the rise, particularly due to lifestyle factors like alcohol consumption and obesity. Gareth Roberts tackled this pressing issue in his blog post on decompensated liver disease, which is becoming increasingly common in emergency departments (EDs) across the UK and beyond.
Gareth outlines a comprehensive care bundle designed to manage patients with decompensated liver disease effectively. This bundle includes seven key points:
-
Thorough Investigation: Quick and accurate investigations are essential, particularly for detecting complications like spontaneous bacterial peritonitis (SBP), which can be life-threatening.
-
Infection Management: Aggressive treatment of infections is critical, with a focus on using appropriate antibiotics and monitoring for SBP.
-
Acute Kidney Injury (AKI) and Hyponatremia: These complications are common in liver disease patients and must be managed carefully. Gareth discusses the potential benefits of human albumin in these cases.
-
GI Bleeding: Gastrointestinal bleeding, especially from varices, poses a significant risk. Gareth directs readers to additional resources on St Emlyn’s, including a presentation by Chris Gray on managing GI bleeding.
-
Hepatic Encephalopathy: This condition can severely alter a patient’s mental status and requires careful management. With the increasing prevalence of liver disease, understanding and managing hepatic encephalopathy is more important than ever.
Gareth’s post is a must-read for anyone dealing with liver disease in the ED, providing both practical advice and links to further resources.
Expanding Education: The MSc in Emergency Medicine
Education is a cornerstone of St Emlyn’s, and we’re excited to announce the expansion of the MSc in Emergency Medicine at Manchester Metropolitan University. This program has been running successfully for several years and is now broadening its scope to include paramedics, making it a truly multi-professional and multi-disciplinary course.
The MSc program offers a variety of modules tailored to the specific needs of different healthcare professionals. Whether you’re looking to deepen your clinical knowledge, enhance your leadership skills, or explore new areas of emergency medicine, this program has something to offer. For more details, visit our website or reach out directly.
Supporting St Emlyn’s: Keep Our Content Free and Accessible
St Emlyn’s remains committed to providing free and open-access content to the global emergency medicine community. However, maintaining and expanding our offerings requires resources. If you find value in what we provide, please consider supporting us financially. Even a small contribution can help us continue to deliver high-quality content to healthcare professionals worldwide.
Introducing Coda: The Next Evolution After SMACC
Coda is the latest evolution in the SMACC legacy, aiming to broaden the scope of its predecessor by incorporating a wider range of specialties, including oncology, public health, and surgery. As a member of the Coda executive team, I can attest to the ambitious goals of this new conference series.
Coda retains the clinical excellence that SMACC was known for, but with an added emphasis on advocacy. Each year, Coda will tackle a significant global health issue, with the inaugural theme focusing on climate change and its impact on medical practice.
It’s important to note that while climate change is a key focus, it won’t dominate the entire conference. Only about 25% of the program will be dedicated to this theme, with the remaining 75% featuring the high-quality clinical content you’ve come to expect from SMACC. The first Coda conference is set to take place in Melbourne in 2020, and we encourage you to participate, whether in person or remotely.
The Zero Point Survey: A Game-Changer in Resuscitation
The Zero Point Survey, a concept championed by Cliff Reid, is gaining widespread recognition for its transformative impact on resuscitation practices. The idea shifts the focus of the primary survey in resuscitation from when you first encounter the patient to what you do before you even meet them.
This approach emphasizes the importance of preparation—both mental and environmental. By optimizing everything you can control before the patient arrives, you set the stage for delivering high-quality care when it matters most.
Feedback from the EM community has been overwhelmingly positive, with many clinicians reporting that the Zero Point Survey has changed how they manage the resuscitation room. It’s not just a theoretical concept; it’s a practical tool that’s making a real difference in patient outcomes.
If you’re not yet familiar with the Zero Point Survey, I strongly encourage you to explore the resources available on the St Emlyn’s website, including an excellent video by Cliff Reid that outlines the key elements of this approach.
Looking Ahead: What’s Next for St Emlyn’s?
As we wrap up our review of September’s content, it’s clear that the St Emlyn’s team has been hard at work bringing you the latest in emergency medicine education and clinical practice. But there’s much more to come.
In the coming months, we’ll be covering exciting topics at upcoming conferences, including the ArchiEM conference in Gateshead and the Slovenia ERC conference. These events promise to bring fresh insights and new perspectives that we’ll be sharing with you through our blog posts and podcasts.
In the meantime, keep doing the incredible work you do in emergency medicine. It’s a challenging field, but it’s also incredibly rewarding, and you’re making a difference every day. Thank you for being part of the St Emlyn’s community, and I look forward to continuing this journey with you.
Stay tuned for more great content, and as always, keep pushing the boundaries of what’s possible in emergency care.
Monday Oct 14, 2019
Monday Oct 14, 2019
The CRASH-3 Trial: Revolutionizing Head Injury Management with Tranexamic Acid
The CRASH-3 trial, a landmark study in the field of emergency medicine, has brought significant attention to the potential role of tranexamic acid (TXA) in managing traumatic brain injury (TBI). As one of the largest randomized controlled trials ever conducted on head injury patients, its findings could reshape clinical practices globally, particularly in the pre-hospital and emergency department settings.
Overview of the CRASH-3 Trial
The CRASH-3 trial was designed to assess the efficacy of TXA in reducing mortality among patients with traumatic brain injury. TXA is an antifibrinolytic agent commonly used to prevent excessive bleeding in various medical scenarios, such as trauma, surgery, and postpartum hemorrhage. The question posed by CRASH-3 was whether TXA could also reduce deaths in patients who had suffered a TBI, a question that had remained unanswered despite the success of the CRASH-2 trial in managing extracranial bleeding.
Patient Population and Inclusion Criteria
The trial focused on adults aged 16 years and older who had sustained a traumatic brain injury. To be included, patients needed to have either a Glasgow Coma Scale (GCS) score of 12 or lower or a positive CT scan indicating intracranial bleeding. Notably, patients with significant extracranial bleeding were excluded from the trial to specifically measure the effect of TXA on TBI outcomes.
A critical aspect of the trial was the timing of TXA administration. Initially, the protocol allowed TXA to be administered within eight hours of injury. However, as data from other studies like the WOMAN trial and CRASH-2 became available, suggesting that the benefits of TXA diminish after three hours, the protocol was adjusted. This change meant that the majority of patients received TXA within three hours of injury, a key factor in the study's final analysis.
Key Findings of the CRASH-3 Trial
The CRASH-3 trial enrolled 12,737 patients across 29 countries, making it one of the most extensive studies of its kind. The primary outcome measured was all-cause mortality at 28 days post-injury. The results showed that overall mortality was slightly lower in the TXA group (18.5%) compared to the placebo group (19.8%), although this difference was not statistically significant.
However, a pre-specified subgroup analysis provided more compelling evidence. When patients with a GCS of 3 and bilateral unreactive pupils (indicating very severe brain injury) were excluded, TXA demonstrated a more significant benefit. In this subgroup, the mortality rate was 12.5% in the TXA group versus 14% in the placebo group, a statistically significant reduction with a relative risk of 0.89. This finding suggests that TXA is particularly beneficial for patients with moderate head injuries (GCS 9-15) who are more likely to survive if bleeding is controlled.
Number Needed to Treat (NNT)
One of the critical metrics for evaluating the effectiveness of a treatment is the number needed to treat (NNT). In the CRASH-3 trial, the NNT was 67, meaning that 67 patients would need to be treated with TXA to save one additional life at 28 days post-injury. For comparison, the NNT for aspirin in acute myocardial infarction is about 42, which is widely regarded as highly effective. An NNT of 67 is therefore quite favorable in the context of emergency medicine, particularly for a condition as serious as traumatic brain injury.
Timing of Administration
The CRASH-3 trial strongly reinforced the importance of administering TXA as early as possible after a head injury. The data indicated a 10% reduction in TXA’s effectiveness for every 20-minute delay in patients with mild to moderate head injury. This underscores the need for TXA to be administered in the pre-hospital setting, ideally by paramedics at the scene or en route to the hospital. Delaying treatment until after arrival at the emergency department or after conducting a CT scan may significantly reduce the drug's benefits.
Implications for Clinical Practice
The results of the CRASH-3 trial suggest that TXA should be considered for all patients with moderate traumatic brain injury, particularly those with a GCS of 9 to 15 and confirmed intracranial bleeding. For patients with severe head injuries (GCS of 8 or less, or with bilateral unreactive pupils), the benefits of TXA are less clear, likely due to the severity of the primary brain injury.
Given the trial’s findings, it is recommended that TXA be integrated into clinical protocols for the management of head injuries. This is especially relevant in pre-hospital care, where early intervention is possible. TXA should be administered as soon as possible after the injury occurs, particularly in cases where a significant delay in getting to the hospital is expected.
Cost-Effectiveness and Accessibility
Another important aspect of TXA is its cost-effectiveness. In the UK, a 1-gram dose of TXA costs approximately £1, making it an affordable treatment option for healthcare systems worldwide. This low cost makes TXA a viable option not only in high-income countries but also in low- and middle-income countries where healthcare resources are often limited. Given its affordability and the potential to save lives, TXA is an attractive option for widespread use in managing traumatic brain injury globally.
Considerations for Special Populations
Although the CRASH-3 trial focused on adults, there is a strong rationale for extending its findings to pediatric patients. The physiology of traumatic brain injury in children is similar to that in adults, and there is no evidence to suggest that TXA would act differently in a younger population. As such, it would be reasonable to use TXA in children with TBI, following the same dosing guidelines adjusted for body weight.
Future Directions: Intramuscular TXA and Beyond
While CRASH-3 has provided valuable insights, research into TXA’s potential uses continues. One area of interest is the development of intramuscular (IM) TXA, which could be particularly useful in pre-hospital settings where intravenous (IV) access is challenging. The possibility of an auto-injector for TXA is also being explored, which could simplify administration and further broaden its use, especially in resource-limited settings.
Conclusion: Implementing CRASH-3 Findings in Practice
The CRASH-3 trial marks a significant advancement in our approach to treating traumatic brain injury. The evidence strongly supports the use of TXA, particularly in patients with moderate head injuries who receive the drug within three hours of injury. TXA is safe, cost-effective, and easy to administer, making it a valuable tool in both pre-hospital and hospital settings.
The implementation of CRASH-3’s findings into clinical practice could save thousands of lives annually, particularly in settings where early intervention is possible. As the emergency medicine community, we must act swiftly to incorporate these findings into our protocols and training, ensuring that TXA is used effectively to improve outcomes for patients with traumatic brain injury worldwide.
Sunday Oct 06, 2019
Saturday Oct 05, 2019
Friday Sep 27, 2019
Friday Sep 27, 2019
Our latest podcast from the #stemlynsLIVE conference last year. Dan Horner talks on the concept and potential role of the UK Resuscitationist.