
1.2M
Downloads
240
Episodes
A UK based Emergency Medicine podcast for anyone who works in emergency care. The St Emlyn ’s team are all passionate educators and clinicians who strive to bring you the best evidence based education. Our four pillars of learning are evidence-based medicine, clinical excellence, personal development and the philosophical overview of emergency care. We have a strong academic faculty and reputation for high quality education presented through multimedia platforms and articles. St Emlyn’s is a name given to a fictionalised emergency care system. This online clinical space is designed to allow clinical care to be discussed without compromising the safety or confidentiality of patients or clinicians.
Episodes
Saturday Jun 13, 2020
Saturday Jun 13, 2020
Lots to chat about on the podcast this month, and not just COVID! There's been blog posts about clots, troponin and even telly, as well as the Journal Club series.
Keep a look out for the new St Emlyn's Lesson Plans that we hope will help usher in a new era of medical education in a socially distanced world.
If you would like to donate to the fund in the memory Adel Aziz you can find the link here.
We hope you're finding all of our output useful. Please do subscribe to the website (in the top right hand corner) and rate our podcast on iTunes.
Take care
Iain
Podcast edited by Izzy Carley
PS You can find the Lesson Plans here. Still a work in progress, but as you've read these "shownotes" you deserve to have a sneak preview...
Thursday Jun 04, 2020
Thursday Jun 04, 2020
Welcome to our seventh webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn's.
The live event took place on Tuesday 26th May.
Today's panel will be hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar, Prof Pam Vallely (Professor of Medical Virology), Ellie Hothershall (Consultant in Public Health), Prof Simon Carley and special guest Kelly Ann Janssens (Emergency Physician in Ireland) to discuss five papers about COVID-19 infection.
This will be the last weekly journal club, but we will be back with more EBM goodness very soon. Do let us know what you like to be included at stemlyns@gmail.com
References
-
Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 — Preliminary Report. N Engl J Med. Published online May 22, 2020. doi:10.1056/nejmoa2007764
-
Mehra MR, Desai SS, Ruschitzka F, Patel AN. Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis. The Lancet. Published online May 2020. doi:10.1016/s0140-6736(20)31180-6
-
Gray N, Calleja D, Wimbush A, et al. “No test is better than a bad test”: Impact of diagnostic uncertainty in mass testing on the spread of Covid-19. Published online April 22, 2020. doi:10.1101/2020.04.16.20067884
-
Peyrony O, Marbeuf-Gueye C, Truong V, et al. Accuracy of Emergency Department clinical findings for diagnostic of coronavirus disease-2019. Annals of Emergency Medicine. Published online May 2020. doi:10.1016/j.annemergmed.2020.05.022
-
Ludvigsson JF. Children are unlikely to be the main drivers of the COVID‐19 pandemic – a systematic review. Acta Paediatr. Published online May 19, 2020. doi:10.1111/apa.15371
Friday May 22, 2020
Friday May 22, 2020
Welcome to our sixth COVID-19 Journal Club Podcast.
The panel was hosted by Rick Body and included Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar, Prof Pam Vallely (Professor of Medical Virology), Prof Simon Carley and special guest Liz Crowe (Advanced Clinician Social Worker and PhD candidate in health staff wellbeing in Brisbane) to discuss four papers about COVID-19 infection. We were especially pleased to welcome Liz this week, which enabled us to focus on the important topics of grief, loss and communication during the COVID-19 pandemic.
References
Wednesday May 13, 2020
Wednesday May 13, 2020
Over the last few years many of us in the UK have started to incorporate high-sensitivity troponin into the assessment of patients presenting with chest pain.
We have seen these samples taken at ever shorter intervals, aiming to discharge low risk patients safely, sooner from the Emergency Department (ED). This has been driven in part by the "Four Hour Emergency Access Target" as well as increased crowding in overwhelmed EDs.
In this podcast, internationally renowned researcher Prof Rick Body discusses the latest in troponin research and the recent LoDED study.
The Shownotes
The various organisations mentioned by Rick can be found here:
The Innovation Agency Webinar Series
The NHS Accelerated Access Collaborative
The CQUIN that will be implemented later this year (page 15 for the Troponin section)
The Draft NICE recommendations
Thursday May 07, 2020
Thursday May 07, 2020
Welcome to our fourth webinar and journal club reviewing recent research and featuring COVID-19 updates, hosted by the University of Manchester, Manchester Royal Infirmary and Royal College of Emergency Medicine in collaboration with St Emlyn's.
The live event tool place on Tuesday 5th May at 11.30am BST (10.30am GMT).
The panel was again be hosted by Rick Body The panel includes Prof Paul Klapper (Professor of Clinical Virology), Dr Charlie Reynard (NIHR Clinical Research Fellow), Dr Anisa Jafar (Academic Clinical Lecturer), Prof Pam Vallely (Professor of Medical Virology), Prof Simon Carley and special guest Justin Morgenstern to discuss six papers about COVID-19 infection.
There will be another COVID 19 Journal Club next week (Tuesday 12th May at 11am).
References
Podcast edited from a live webinar by Izzy Carley
Sunday May 03, 2020
Sunday May 03, 2020
It's been another busy month at St Emlyn's, with the publication of 15 blog posts and five podcasts, but there does seem to be an awful lot to talk about!
Of course there have been multiple posts and podcasts about COVID-19, and you can fiind all of these on our special St Emlyn's page. Highlights have included the three RCEM/St Emlyn's Webinars which we are delighted to host in podcast form.
It's not just been coronavirus though, we have also dipped out toes into exercise and nutrition, graphic design and horticulture!
Parts of the site have also undergone a bit of a redesign with the curriculum pages now easier to navigate to find that post to fioll an e-portfolio hole.
We hope you're finding all of our output useful. Please do subscribe to the website (in the top right hand corner) and rate our podcast on iTunes.
They'll be much more to come in May I am sure.
Take care
Iain
Podcast edited by Izzy Carley
Wednesday Apr 22, 2020
Wednesday Apr 22, 2020
In this podcast, Dan and Iain talk about the clinical journey of a COVID-19 patient, beyond the ED, with insights from the critical care unit. There are some concepts here that we don’t have time to do full justice to in the podcast, so there is a comprehensive set of "show notes" and all the references at www.stemlynsblog.org/covid-19-and-critical-care
Sunday Jan 19, 2020
Sunday Jan 19, 2020
Our regular round up of the best of the blog from December 2019. Published a little late, largely because of Coronavirus issues and general business.
Thursday Nov 14, 2019
Thursday Nov 14, 2019
Simon and Zaf talk about the practicalities of REBOA and discuss whether it's ready for prime time in the UK.
Introduction
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) is a minimally invasive technique designed to control hemorrhage in patients with life-threatening bleeding and offers a bridge to definitive surgical intervention. Here at St Emlyn’s, we are committed to exploring innovative solutions that enhance patient outcomes in emergency medicine. In this post, we delve into the essentials of REBOA, its clinical application, benefits, and challenges.
Understanding REBOA
REBOA involves the insertion of a balloon catheter into the aorta via the femoral artery. By inflating the balloon, we can occlude the aorta, thus controlling bleeding below the point of occlusion. This procedure is particularly useful in cases of non-compressible torso haemorrhage, where traditional methods of haemorrhage control are inadequate.
Indications and Contraindications
Indications:
- Hemorrhagic shock from pelvic fractures or abdominal bleeding.
- Trauma patients with signs of severe hemorrhage unresponsive to fluid resuscitation.
- As a temporary measure until surgical control of bleeding is achieved.
Contraindications:
- Patients with known aortic pathology (e.g., aortic dissection).
- Significant injury above the diaphragm.
- Prolonged transport times where REBOA may not be beneficial.
The Procedure
Preparation
Before performing REBOA, it is crucial to ensure that the patient is appropriately resuscitated and stabilized as much as possible. This includes securing the airway, ensuring adequate ventilation, and achieving initial hemodynamic stabilization.
Insertion and Inflation
- Vascular Access: Gain access to the common femoral artery using ultrasound guidance to minimize complications.
- Catheter Insertion: Insert the REBOA catheter through a sheath into the femoral artery. Advance the catheter under fluoroscopic or ultrasound guidance to the desired level in the aorta (Zone I: above the celiac artery for abdominal hemorrhage, Zone III: above the bifurcation of the iliac arteries for pelvic hemorrhage).
- Balloon Inflation: Inflate the balloon to occlude the aorta. This temporarily controls bleeding and allows time for definitive surgical repair.
Monitoring and Maintenance
Continuous monitoring of vital signs and catheter position is essential. The occlusion time should be minimized to reduce ischemic complications. Ideally, REBOA should serve as a bridge to definitive surgical intervention within 30-60 minutes.
Benefits and Challenges
Benefits
- Rapid Hemorrhage Control: REBOA can quickly control bleeding, buying crucial time for surgical intervention.
- Less Invasive: Compared to traditional open thoracotomy with aortic cross-clamping, REBOA is less invasive, reducing associated morbidity.
- Improved Survival Rates: Emerging evidence suggests that REBOA can improve survival rates in appropriately selected trauma patients.
Challenges
- Technical Expertise: REBOA requires specific training and expertise. Improper technique can lead to significant complications.
- Ischemic Complications: Prolonged aortic occlusion can lead to ischemia of distal organs and tissues, necessitating careful monitoring and timely deflation.
- Resource Intensive: REBOA demands resources such as fluoroscopy, ultrasound, and trained personnel, which may not be available in all settings.
Conclusion
REBOA represents a promising advancement in trauma care, offering a vital tool in the management of life-threatening haemorrhage, but it's utility in the Emergency Department is uncertain.
Further reading
Thursday May 30, 2019
Thursday May 30, 2019
Alan Grayson takes us through his thoughts on ATLS. Is it really as terrible the #FOAMed world makes out?
Sunday May 19, 2019
Sunday May 19, 2019
This is the podcast that links to the following two posts on how to deal with some of the hardest events we have to deal with in emergency and critical care.
You can read more about the topic on the following two blogs.
https://www.stemlynsblog.org/wellbeing-for-the-broken-part-1-liz-crowe-for-st-emlyns/
https://www.stemlynsblog.org/wellbeing-for-the-broken-part-2-st-emlyns/
This is a tough listen so if you are affected by the content do chat through with colleagues.
Wednesday Apr 10, 2019
Wednesday Apr 10, 2019
Back in late 2018 we gathered in Manchester for the inaugural #stemlynsLIVE conference. Our friend Dr George Wills gave a great talk on Aortic Emergencies.
All emergency physicians know that it's all to easy to miss an aortic catastrophe. Listen to George's wisdom on common pitfalls and top tips to make you a better emergency clinician.
vb
S
Also check out these excellent #FOAMed resources.
- Subscribe to the blog (look top right for the link)
- Subscribe to our PODCAST on iTunes
- Follow us on twitter @stemlyns
- PLEASE Like us on Facebook
- Find out more about the St.Emlyn’s team
Friday Jan 11, 2019
Friday Jan 11, 2019
This podcast and presentation was recorded at the St Emlyn's LIVE conference in Manchester 2018. In this presentation Clare takes us through the rationale, principles, training and practice that we need in order to continually develop as prehospital and resuscitation practitioners.
You can read more from the event at http://www.stemlynsblog.org
This is a great presentation for anyone interested in continually developing their own and their colleagues practice, delivered by someone who really knows what they are talking about and who works for one of the best developed resuscitation services in the world.
Clare is an Emergency Physician and specialist in Pre-Hospital Care and Retrieval medicine based in Sydney, with Royal Prince Alfred Hospital and Sydney HEMS. She has completed a fellowship in simulation based education, and enjoys training with “real” people - patients, bystanders and the other clinicians we come across as we treat our patients every day. She is a lecturer with the University of Sydney, and is involved in education for the NSW Institute for Trauma Injury Management. When Clare is not working on helicopters or training teams, she is studying yoga or hanging out with her puppy, Archie.
Sunday Dec 23, 2018
Sunday Dec 23, 2018
November was a busy month for the St Emlyn's team with a variety of blogs on conferences, EBM, philosophy and education. Here's the podcast and the links to the blogs mentioned in November.
Wednesday Nov 28, 2018
Wednesday Nov 28, 2018
Salim Rezaie from the REBEL EM podcast takes us through the optimal management of cardiac arrest and also explores some of the controversies and difficulties that make the difference to our patients.
You can read a lot more about the background to this talk, see the evidence and watch the video on the St Emlyn's site. Just follow this link. https://www.stemlynsblog.org/beyond-acls-salim-rezaie-at-stemlynslive/
Sunday Oct 28, 2018
Sunday Oct 28, 2018
This presentation was given at the inaugural #stemlynsLIVE conference on the 8th of October 2018 in Manchester. You can read more about the presentation and the conference here. https://www.stemlynsblog.org/in-pursuit-of-excellence/
Tuesday Apr 24, 2018
Tuesday Apr 24, 2018
Iain and Simon review the best of the blog from February 2018.
Simon Carley
Monday Apr 02, 2018
Monday Apr 02, 2018
Iain and Simon round up the blog posts from January 2018. You can listen to the podcast below. Links to all the blog posts mentioned are listed below.
As 2017 ends and we look forward to 2018 it’s time to reflect on a year with the St.Emlyn’s team. Despite our chronological and geographical dispersal it’s really felt like a team effort in 2017. We have travelled, learned, listened,…
Read more
JC: Devastating Brain Injury. Complex decisions in the resus room. St.Emlyn’s
January 4, 2018 3 Comments Social media can sometimes give the impression that all is rosy in the world of resuscitation. We hear of the amazing saves, the wonders of ECMO, helicopters and heroic acts with great outcomes, but the reality is of course very…
Read more
[caption id="attachment_31228" align="alignleft" width="300"] northern emergency medicine conference[/caption]
northern emergency medicine conference[/caption]
St.Emlyn’s goes further north – NEM Conference #NEMC18
January 9, 2018 0 Comments It’s the second time I’ve been to the Northern Emergency Medicine conference, this year held in the sunny city of Durham. I say sunny… I needed my jacket. Last year’s programme was great and included some fantastic speakers, including our…
Read more
JC: Can I safely discharge dizzy patients from the ED?
January 12, 2018 4 Comments Last month, I came across a clinical review published in the Annals of Emergency Medicine1 that got me really excited! It got me excited (in a geeky professional sense of course…) as it covered a topic that causes significant…
Read more
On Reflection

January 16, 2018 3 Comments On Reflection I’ve been reflecting on reflection for some time now, at least since I started formally collecting my lessons from Sydney HEMS and probably even before that, because this sort of meta nonsense is something medical education enthusiasts like…
Read more
CRYOSTAT-2 with Ross Davenport
January 21, 2018 2 Comments You might be aware that an exciting new trial has started called Cryostat-2. This is exciting as it has the potential to improve patient outcomes, but also because it will involve all the Major Trauma Centres in England and 8…
Read more
 The End of the ‘Roid? JC: ADRENAL
The End of the ‘Roid? JC: ADRENAL
January 22, 2018 4 Comments So another year, another Critical Care Reviews meeting. Rob is doing an absolutely fantastic job with these, inviting lead authors from major critical care trials to present and defend their work. In fact, this is going so well that this…
Read more
Belgian EM at BeSEDiM 2018.
January 28, 2018 0 Comments Last weekend, the BeSEDiM (Belgian Society of Emergency and Disaster Medicine) organised their annual symposium. It is the scientific organization of the Belgian emergency physicians with Said Idrissi as chairman. 13 years ago, Belgian Emergency medicine was born as a…
Read more
 Is there anything else I need to know? Working in Africa.
Is there anything else I need to know? Working in Africa.

January 29, 2018 0 Comments This is a guest post from our good friend Stevan Bruijns aka @codingbrown Stevan has been an advocate of international emergency medicine for many years and he, like us feels that there is much that high income countries can do…
Read more
vb
S
Before you go please don’t forget to…
- Subscribe to the blog (look top right for the link)
- Subscribe to our PODCAST on iTunes
- Follow us on twitter @stemlyns
- See our best pics and photos on Instagram
- PLEASE Like us on Facebook
- Find out more about the St.Emlyn’s team
Simon and Iain belatedly reflect on a tough winter and the posts in January.
Check out stemlynsconference.com if you want to know more about #StEmlynsLIVE
S
Wednesday Jan 24, 2018
Wednesday Jan 24, 2018
In this podcast Simon talks to Dan Harvey (ITU) and Mark Wilson (Neurosurgeon) on the management of complex patients with a perceived devastating brain injury.
This podcast is linked to the blog on the St.Emlyn's website.
http://stemlynsblog.org/jc-devastating-brain-injury-complex-decisions-in-the-resus-room-st-emlyns/
S
Wednesday Aug 02, 2017
Wednesday Aug 02, 2017
St.Emlyn's is a virtual hospital based in Virchester.
In reality we are a team of Emergency Physicians, friends and colleagues interested in medical education, emergency medicine and critical care. We blog because education matters. Our numbers are growing every day... please feel free to contact us.
Senior Editors
 Professor Simon Carley FOAM(Ed) Professor Simon Carley FOAM(Ed)Professor of Emergency Medicine, Manchester Metropolitan University; Consultant in Emergency Medicine. Co- founder of BestBets, StEmlyns, MSc in EM and other stuff. Research interests in diagnostics, MedEd, Major incidents & Evidence based Emergency Medicine. *Read Posts* |
|
|
|
 Professor Rick Body MB ChB, MRCSEd(A&E), FCEM, PhD Professor Rick Body MB ChB, MRCSEd(A&E), FCEM, PhDConsultant in Emergency Medicine at Manchester Royal Infirmary and Honorary Lecturer in Cardiovascular Medicine at the University of Manchester. Major research interests are in the early diagnosis of acute coronary syndromes and humane approaches to improving patient well-being in the ED. Methodological expertise in clinical decision rules, diagnostic studies and cohort studies. - Research - Blog - *Read Posts* |
|
|
|
Editorial Board
 Dr Natalie May MBChB, MPHe, MSc, MCEM, FCEM Dr Natalie May MBChB, MPHe, MSc, MCEM, FCEMConsultant Emergency Physician with speciality training in Paediatric Emergency Medicine, currently working in Prehospital and Retrieval Medicine at Sydney HEMS. Numerous interests in medical education, leadership and emergency paediatrics. #FOAMaoke queen, obsessed with running. *Read Posts* |
|
|
|
 Dr Iain Beardsell FOAM(Ed) Dr Iain Beardsell FOAM(Ed)Consultant in Emergency Medicine and Clinical Lead, University Hospitals Southampton and HIOWW HEMS doctor. A passionate advocate for EM with a cup that is (almost) always half full. *Read Posts* |
|
|
|
 Dr Alan Grayson Dr Alan GraysonGrumpy, balding Yorkshireman, who despite practising medicine on the good folk of Manchester and its environs, still lives in god's own county, after a brief sabbatical learning medicine in Edinburgh and then training in EM in Newcastle and NW England. Has an unhealthy interest in bikes, pies, cricket and Huddersfield Town FC. *Read Posts* |
|
| |
 Dr Richard Carden BSc, MSc, MBChB, MRCEM, RAMC(V) Dr Richard Carden BSc, MSc, MBChB, MRCEM, RAMC(V)Emergency Medicine trainee. Captain in the Royal Army Medical Corps. (Reserves). Former MSc Trauma Sciences (Military and Austere) student, impending Centre for Trauma Sciences PhD student, current Diploma in Medical Care of Catastrophes student. Interested in trauma, toxicology, psychology, physiology and critical care. Trainee rep on the St.Emlyn's team. *Read Posts* |
| ||
 Dr Janos Peter Baombe MD FRCEM FEBEEM PgCert MSc Dr Janos Peter Baombe MD FRCEM FEBEEM PgCert MScEmergency medicine consultant, Manchester Royal Infirmary. Fellow of the Royal College of Emergency Medicine. Passionate about european EM networks, infectious disease outbreaks and ED preparedness, ultrasonography. World traveller and keen sportsman. *Read Posts* |
| ||
 Liz Crowe BSW PhD Candidate Liz Crowe BSW PhD CandidateAdvanced Clinician Social Worker who has worked extensively in ED and PICU. Specialises in counselling children,families and staff impacted by loss, trauma, crisis and bereavement. Doing a PhD on Staff Wellbeing in Critical Care. Author of 'The Little Book of Loss and Grief You Can Read While You Cry'. Enjoys Gallows Humour. *Read Posts* |
|
| |
 Dr Chris Gray BSc MBBS MRCP MRCEM Dr Chris Gray BSc MBBS MRCP MRCEMEmergency Medicine trainee at the Royal Manchester Children's Hospital. Interested in pre-hospital care, trauma, and critical care. Keen educator, musician and cake-maker. *Read Posts* |
|
| |
 Ashley Liebig RN Ashley Liebig RNVet 101st Airborne combat medic. Flight Nurse & Helicopter Rescue Specialist. ECMO enthusiast. |
|
| |
 Dr Laura Howard Dr Laura HowardJunior doctor in Virchester. Interested in mountain bikes, resuscitation, trauma and critical care. *Read Posts* |
| ||
 Mr Ross Fisher Mr Ross FisherConsultant Paediatric Surgeon at Sheffield Children's Hospital and Chairman of TARNlet. Visiting lecturer in Virchester and basically anywhere else that will pay bus fare. Owns more Moleskine notebooks than is healthy, most of them full of ideas on #presentationskills Passionate convert to all things #FOAMy *Read Posts* |
|
|
|
 Dr Dan Horner BA, MBBS, MRCP, MCEM, FRCEM Dr Dan Horner BA, MBBS, MRCP, MCEM, FRCEMConsultant Emergency Physician at Salford Royal Hospitals Trust with subspecialty training in Intensive Care Medicine. Researcher with specialist interest in EBM and thromboembolic disease. New to all this blogging and tweeting, but old to the general chaos and lividity of the Emergency Department. An interest in VTE, Critical Care and a bit of trauma now and then. Also trying to stay sane while being overworked and underpaid. *Read Posts* |
Contributors
 Dr Gareth Hardy Dr Gareth HardyEmergency Medicine trainee with a long running and excellent blog. Thinks beyond the superficial and constantly questions the evidence for what we do.(Ed - A great asset and probably the only person here who knows what he's doing!) *Read Posts* |
|
|
|
 Dr Craig Ferguson FCEM Dr Craig Ferguson FCEMEmergency physician, Manchester Royal Infirmary. Interests in medical technology, resuscitation and medical research. Research interests in the diagnosis of acute heart failure in the ED. Fellow of the College of Emergency Medicine. *Read Posts* |
|
Monday May 15, 2017
Monday May 15, 2017
A critical appraisal nuggest on simple ways to understand the true effect of an intervention. Also see this more in depth podcast done with Iain Beardsell
http://ebem.podbean.com/2011/11/03/statistics-2/
vb
S
Sunday Mar 05, 2017
Sunday Mar 05, 2017
In a new podcast format Simon (@EMManchester) and Iain (@docib) discuss the month's offerings from the St Emlyn's blog and podcast (www.stemlynsblog.org).
It's been a month full of interesting posts on subjects as diverse as Thrombolysis in Stroke (Alan Grayson), The Future of Emergency Medicine in the Social Age (Simon), Cardiac Arrest Centres (Simon), Love in Critical Care (Liz Crowe), Transfers (Nat and Simon), Thrombolysis in PE (a guest post from FOAMed legend Anand Swarminathan) and Benzos in Back Pain (Janos). Head to the website for the articles themselves and all the references and links you need.
We're aiminig to make this a regular monthly podcast - let us know if it's useful and enjoyable and how we could make it even more educational.
Saturday Jan 14, 2017
Saturday Jan 14, 2017
Rick and Simon talk about the merits of prospective and retrospective studies
Thursday Nov 17, 2016
Thursday Nov 17, 2016
A quick round up of events from the excellent Teaching Course in New York (https://flippingmeded.com/) with guests Ross Fisher (@ffoliet), Ashley Leibig (@ashleyliebig), Sandra Viggers (@StarSkaterDK) and Camilla Sorenson (@Camillabirgitte).
For brilliant summaries of each day, with details from every talk, visit http://scanfoam.org/teaching-course-nyc-day-1-ttcnyc16/ (Day 1) and http://scanfoam.org/teaching-course-nyc-day-2-ttcnyc16/ (Day 2)
Sunday Jul 31, 2016
Sunday Jul 31, 2016
Part 2 of our podcasts on major trauma handovers. This follows on from the discussion at SMACC and is intended to operationalise the concepts we talked about then. This is aimed at a UK audience but should apply pretty much anywhere. So hands off, eyes open and listen in, here we go.
Friday Jul 08, 2016
Friday Jul 08, 2016
Whilst we were in Dublin at the SMACC conference we took the opportunity to get some great minds together on the subject of ED handover at the point between prehospital and hospital teams for the critically ill or injured patient in the resus room.
This is an area of some difficulty in many areas (prob shouldn't be, but it is) and we thought it would be fun and useful to get perspectives from both sides.
As ever, we are not here to be definitive and your service may have a fantastic model that works well. This podcast is to help you think about what you're doing and to consider whether it can be improved.
Doug Lynch is a retrieval doctor from Australia
Ashley Voss-Liebig is a flight nurse from Texas
Natalie May is a retrieval doctor from Sydney (Virchester Alumnus)
Rusty Carroll is a senior paramedic from Virchester and a great supporter of the ATACC group.
We don't have all the answers, but we do have the ideas.
In Virchester it can certainly be improved.....
Tell us what you think and keep an eye out for the blog post on the same subject coming soon.
vb
S
Wednesday Dec 09, 2015
Wednesday Dec 09, 2015
Our summary of Day 2 of the excellent London Trauma Conference. A unique threesome from Nat, Simon and Iain.....
Tuesday Dec 08, 2015
Tuesday Dec 08, 2015
Greetings from the London Trauma Conference!
As has become our pre-Christmas custom, Iain and I have been hanging out at the fabulous London Trauma Conference, hearing about advances and controversies in trauma care and tracking down some of the speakers to find out exactly what they really think (and recording it, for podcasts we'll release in due course).
The conference extends over four days, incorporating the Air Ambulance and Prehospital Day and the Cardiac Arrest Symposium; unfortunately we can't stick around for those but our colleagues over at the RCEM FOAM network will be podcasting from those days too, so keep an eye on their site and podcast feed too.
Saturday Nov 28, 2015
Saturday Nov 28, 2015
My talk from the RCEM conference in Manchester 2015.
Linked blog post here. http://stemlynsblog.org/making-good-decisions-in-the-ed-rcem15/
Slides are here http://www.slideshare.net/simoncarley7/making-good-decisions-rcem-2015-manchester-wednesday
Have fun and enjoy your emergency medicine.
S
Thursday Jun 04, 2015
Thursday Jun 04, 2015
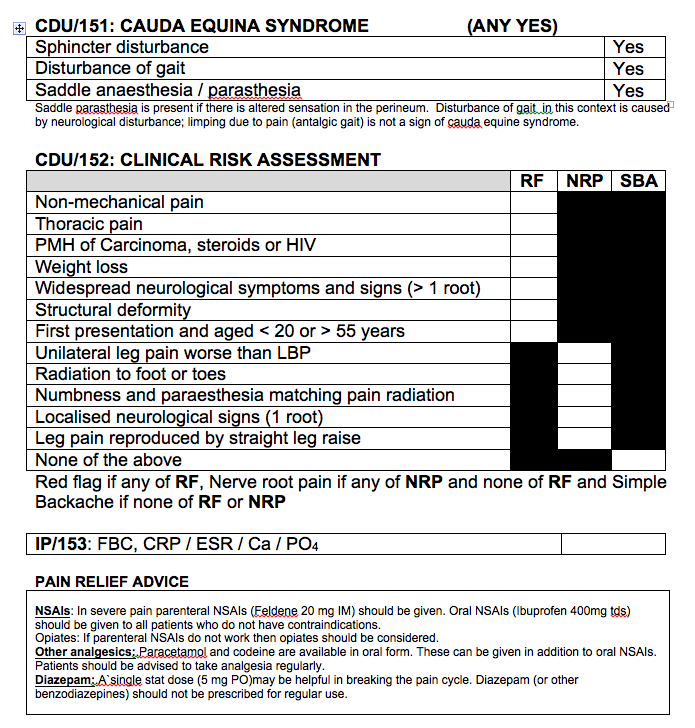
Another induction podcast on a common condition in the ED. Back pain in the ED - it's not all musculoskeletal and there are some really risky diagnoses out there that you need to think about.
Don't forget to listen to Iain's talk on chronic pain link here. https://vimeo.com/97811644
Red flag symptoms and analgesia advice below.
Saturday Apr 18, 2015
Saturday Apr 18, 2015
Iain interviews the wonderful Tim Draycott on the management of the Obstetric patient with trauma.Tim is a consultant Obstetrician from Bristol and is a great speaker on this rather terrifying topic!
Thursday Mar 26, 2015
Thursday Mar 26, 2015

A short podcast updating the UK Advanced Paediatric Life Support (APLS) course guidelines for the management of trauma in children.
Don't forget to read the blog post here. APLS Updates: New kids on the block,
vb
S
Sunday Mar 22, 2015
Sunday Mar 22, 2015
In this podcast he gives us a paediatric perspective on how we should approach the seriously injured child.
Great stuff, controversial in places, challenging to adult dogma and always excellent.
S
PS. If you ever get to hear him speak.... then do, he's awesome. Check this out.
Friday Feb 27, 2015
Friday Feb 27, 2015
 Simon and Iain debate how the management of opiate OD has changed in the ED.
Simon and Iain debate how the management of opiate OD has changed in the ED.
Surely you're not still giving massive doses of naloxone IV and IM are you? Really? Maybe this will make you think again.
vb
S
Sunday Feb 22, 2015
Sunday Feb 22, 2015
Do you think you're awesome at assessing shock?
Think again!
The stupendous Prof Tim Harris (who St.Emlyn's loves) tells us that all is not quite as it seems.....
Listen, learn, be awesome.
vb
S
Wednesday Jan 14, 2015
Wednesday Jan 14, 2015
Managing Early Pregnancy Problems in the Emergency Department
Welcome to the St. Emelene's induction podcast. I'm Iain Beardsell, and I'm Natalie May. Today, we're discussing the management of early pregnancy problems in female patients presenting to the emergency department (ED). Some of you may rarely encounter these cases, while others may see them frequently. This podcast aims to provide a detailed guide on how to manage these patients effectively, optimizing our approach for better patient outcomes.
Understanding Early Pregnancy Problems
Early pregnancy problems can range from minor concerns to life-threatening emergencies. As emergency physicians, our primary goal is to identify and manage the worst-case scenarios promptly. In this post, we'll cover the following topics:
- Worst-case scenarios and initial steps
- History and physical examination
- Risk factors for ectopic pregnancy
- Diagnostic testing: urine vs. serum HCG
- Per vaginal (PV) examination: when to perform
- Management of threatened miscarriage
- Patient communication and support
Worst-case Scenarios and Initial Steps
In emergency medicine, we often think about the worst-case scenarios first. For early pregnancy problems, the most critical concern is an ectopic pregnancy. Ectopic pregnancies occur in about 1 in 100 pregnancies in the UK and can be life-threatening if not identified and treated promptly.
Initial Steps
When a young female patient presents with lower abdominal pain or spotting and is potentially pregnant, our first steps should include:
- Confirming pregnancy status: Use a urine pregnancy test initially.
- Assessing vital signs: Look for signs of hemodynamic instability, such as hypotension or tachycardia, which could indicate a ruptured ectopic pregnancy.
- Taking a detailed history: Understand the patient's symptoms, last menstrual period, and any previous gynecological issues.
History and Physical Examination
A thorough history and physical examination are crucial in managing early pregnancy problems. Here's what you need to focus on:
History
- Last Menstrual Period (LMP): Helps estimate the gestational age.
- Symptoms: Type and location of pain, nature of bleeding, and presence of other symptoms like dizziness or shoulder pain.
- Previous Pregnancies: Gravida (number of pregnancies) and Para (number of completed pregnancies).
- Risk Factors: Previous ectopic pregnancy, pelvic inflammatory disease, and any surgeries or procedures involving the reproductive organs.
Physical Examination
- Abdominal Examination: Look for tenderness, guarding, or rebound tenderness.
- Vital Signs: Monitor for signs of shock or hemodynamic instability.
- Pelvic Examination: In specific cases, to assess for cervical motion tenderness, adnexal tenderness, or masses.
Risk Factors for Ectopic Pregnancy
Understanding the risk factors for ectopic pregnancy can help identify patients who need urgent evaluation. Risk factors include:
- History of pelvic inflammatory disease (PID)
- Previous pelvic or abdominal surgery
- Use of intrauterine devices (IUDs)
- Previous ectopic pregnancy
- Assisted reproductive techniques like IVF
- Anatomical abnormalities of the fallopian tubes or uterus
- Endometriosis
- Use of the progesterone-only pill
Diagnostic Testing: Urine vs. Serum HCG
Determining the pregnancy status and ruling out ectopic pregnancy requires accurate diagnostic testing. Here's a comparison between urine and serum HCG tests:
Urine HCG Test
- Sensitivity: About 96%, particularly when HCG levels are above 100.
- Specificity: High, meaning a positive result is reliable.
- Limitations: May give false negatives if HCG levels are very low, as seen in some ectopic pregnancies.
Serum HCG Test
- Sensitivity and Specificity: Both close to 100%, making it the preferred test for confirming pregnancy and assessing HCG levels.
- Usage: Particularly useful when urine tests are negative but clinical suspicion remains high.
When to Perform a Per Vaginal (PV) Examination
The necessity of PV examinations in the ED can be debated. However, they are essential in specific situations:
- Retained Foreign Bodies: Such as condoms or tampons.
- Significant Vaginal Bleeding: Particularly in cases of suspected cervical shock due to retained products of conception.
For other scenarios, PV examinations are best left to gynecology specialists who have the expertise and appropriate setting to perform these exams with the required sensitivity and specificity.
Management of Threatened Miscarriage
A threatened miscarriage involves vaginal bleeding in a pregnancy less than 24 weeks, with a closed cervical os. It is a common issue that can cause significant anxiety for patients. Here's how to manage these cases:
Terminology
- Threatened Miscarriage: Vaginal bleeding with a closed cervical os.
- Inevitable Miscarriage: Open cervical os, indicating that miscarriage is likely to proceed.
- Complete Miscarriage: All products of conception have passed.
- Incomplete Miscarriage: Some products remain, requiring further management.
Approach
- Assess Bleeding: Light bleeding can often be managed on an outpatient basis. Heavy bleeding requires immediate gynecological consultation.
- Provide Reassurance: Explain that early pregnancy bleeding is common and not necessarily indicative of a miscarriage.
- Pain Management: Offer analgesia, such as paracetamol or cocodamol, to manage discomfort.
- Follow-up: Arrange for follow-up with an early pregnancy assessment unit (EPAU) within 48 hours.
Patient Communication and Support
Dealing with early pregnancy problems can be distressing for patients. Effective communication and support are crucial.
Tips for Communication
- Be Empathetic: Understand that this might be a significant and emotionally charged situation for the patient.
- Explain Clearly: Provide information about what is happening and what the next steps are.
- Avoid Definitive Statements: Unless certain, avoid saying that the patient has definitely miscarried.
- Offer Reassurance: Reiterate that early pregnancy complications are common and often not due to anything the patient did wrong.
Psychological Support
- Acknowledge Emotions: Recognize the patient's feelings and provide support.
- Encourage Support Systems: Suggest involving family or friends for emotional support.
- Professional Help: Refer to counseling services if needed.
Conclusion
Managing early pregnancy problems in the ED requires a systematic approach, starting with identifying worst-case scenarios and performing appropriate diagnostic tests. Understanding the risk factors for ectopic pregnancy and knowing when to perform a PV examination are crucial. Providing compassionate care and clear communication can help support patients through what can be a distressing time.
By optimizing our approach, we can ensure better outcomes for our patients and provide the best possible care in these challenging situations. Always consult senior colleagues when in doubt and follow local guidelines to ensure consistency and quality of care.
Tuesday Jan 06, 2015
Tuesday Jan 06, 2015
First of our podcasts from the London Trauma Conference.
A fantastic episode with Iain talking to Gareth Davies (from London HEMS) talking about Impact Brain Apnoea.
vb
St.Emlyn's
Thursday Dec 11, 2014
Thursday Dec 11, 2014
It's prehospital and helicopter day at #LTC2014! Iain and guest podcaster Caroline Leech chat through the key points of the day.
Saturday Nov 29, 2014
Wednesday Nov 12, 2014
Wednesday Nov 12, 2014
The Challenge and Value of Research in Emergency Medicine: at DGINA 2014
Rick Body's talk from DGINA on the need for research in EM.
Check out the associated blog post at http://stemlynsblog.org
Friday Oct 31, 2014
Friday Oct 31, 2014
Iain and Simon talk about the upcoming SMACC conference in Chicago and do their very best to persuade you to come to the best conference in the world
Friday Oct 31, 2014
Friday Oct 31, 2014
Simon and Nat with a linked podcast to the blog post on the ingestion of button batteries by children.
http://stemlynsblog.org/button-batteries/
S
Tuesday Oct 28, 2014
Tuesday Oct 28, 2014
Simon and Iain discuss what might appear to be a rather dull subject, but it's not. Coding is a key to developing your department and also to secure the functions of UK emergency departments.
A great primer for everyone coming up to FCEM and to anyone interested in how Emergency Departments are funded in the UK.
Follow this link to the associated blog post http://stemlynsblog.org/show-money/
vb
S
Tuesday Sep 23, 2014
Tuesday Sep 23, 2014
Vic Brazil of #FOAMed and #SMACC fame came to talk to the St.Emlyn's team in Virchester.
Listen in for top tips on looking great and sounding super.
vb
S
Friday Sep 12, 2014
Friday Sep 12, 2014
John Hell is a Neurointensivist at University Hospital Southampton and very kindly gave up an afternoon to record his thoughts and share his considerable wisdom about Diffuse Axonal Injury.
I also managed to get him to discuss some other topics including the choice of induction agents and intravenous fluids in patients with head injury.
Please listen, enjoy and comment. We'd love to hear from you, and don't forget to visit the blog site for additional information, slides and content.
vb
Iain Beardsell
Friday Aug 22, 2014
Friday Aug 22, 2014
Understanding Syncope: A Comprehensive Guide for Emergency Medicine
Introduction
Today, we are discussing syncope, a common yet complex condition involving a transient loss of consciousness due to a temporary reduction in blood flow to the brain. This comprehensive guide aims to provide insights into diagnosing and managing syncope in the emergency department.
The Challenge of Syncope Diagnosis
When patients present with collapse, it’s essential to differentiate between mechanical falls and syncope due to physiological reasons. The key to diagnosis lies in understanding whether the event was caused by a transient loss of consciousness or a mechanical fall. This distinction guides the diagnostic pathway and ensures the appropriate management of potential life-threatening conditions.
Physiology of Syncope
Syncope results from a temporary reduction in cerebral perfusion pressure, which can occur due to various physiological disruptions. Understanding the factors affecting cerebral perfusion, such as mean arterial pressure, cardiac output, and peripheral resistance, is crucial. Any significant deviation in these parameters can lead to syncope.
Cardiac Causes of Syncope
Rhythm Issues
Cardiac syncope often involves rhythm disturbances like bradycardia (abnormally slow heart rate) or tachycardia (abnormally fast heart rate). Bradycardia can reduce cardiac output, while tachycardia can decrease stroke volume. Identifying these rhythm issues is vital as they can be life-threatening.
Structural Issues
Structural heart diseases, such as aortic stenosis or hypertrophic cardiomyopathy, restrict blood flow, leading to syncope. Pulmonary embolism, although less common, can also cause syncope by obstructing pulmonary circulation.
Importance of ECG in Diagnosis
The electrocardiogram (ECG) is a critical tool for diagnosing cardiac causes of syncope. It helps identify arrhythmias, conduction abnormalities, and other cardiac issues. Continuous ECG monitoring, or Holter monitoring, can capture transient arrhythmias not seen on a standard ECG.
Neurological Causes of Syncope
Neurological conditions, such as seizures and transient ischemic attacks (TIAs), can present as syncope. Differentiating between these and true syncope is essential. Seizures often have specific signs like tongue biting, loss of bladder control, and post-ictal confusion. TIAs can cause temporary disruptions in blood flow to the brain, leading to syncope-like episodes.
Physiological Causes of Syncope
Vasovagal Syncope
Vasovagal syncope, triggered by stress, pain, or prolonged standing, involves a sudden drop in heart rate and blood pressure. It is a common and generally benign cause of syncope.
Orthostatic Hypotension
Orthostatic hypotension, a drop in blood pressure upon standing, can result from dehydration, medications, or autonomic dysfunction. It is a frequent cause of syncope, especially in elderly patients.
Diagnostic Approach
Patient History
A thorough patient history is crucial for identifying the cause of syncope. Key elements include the circumstances of the episode, prodromal symptoms, witness accounts, and medical history. This information helps distinguish between different causes of syncope.
Physical Examination
A comprehensive physical examination includes checking vital signs, cardiovascular examination, and neurological assessment. Identifying abnormalities during the physical exam can provide clues to the underlying cause of syncope.
Diagnostic Tests
- ECG: Identifies arrhythmias and conduction abnormalities.
- Holter Monitoring: Captures transient arrhythmias.
- Echocardiogram: Assesses structural heart diseases.
- Tilt-Table Test: Diagnoses vasovagal syncope or orthostatic hypotension.
- Blood Tests: Evaluate electrolyte levels, blood glucose, and cardiac biomarkers.
Management Strategies
Cardiac Syncope
Management of cardiac syncope focuses on stabilizing heart rhythm and function. Treatments may include pacemaker implantation for bradycardia, medications for tachycardia, and surgical interventions for structural heart diseases. Arrhythmias may require implantable cardioverter-defibrillators (ICDs).
Neurological Syncope
Managing neurological causes involves addressing the underlying condition. Antiepileptic medications control seizures, while immediate interventions restore blood flow in strokes or control bleeding. TIAs require medications and lifestyle changes to reduce recurrence risk.
Physiological Syncope
- Vasovagal Syncope: Management includes avoiding triggers, increasing fluid and salt intake, and using compression stockings. Severe cases may require medications.
- Orthostatic Hypotension: Gradual position changes, increased hydration, and reviewing medications. Medications like fludrocortisone may be necessary.
- Dehydration: Rehydration with oral or intravenous fluids.
- Medication Review: Adjusting or discontinuing medications contributing to syncope.
Safety Netting and Follow-Up
Safety netting ensures patients receive appropriate follow-up care and instructions. Key elements include providing clear discharge instructions, scheduling follow-up appointments, and educating patients about syncope causes and management.
Special Considerations
Reflex Anoxic Seizures
Reflex anoxic seizures, seen especially in children, involve shaking movements due to a drop in oxygenation. These can be misinterpreted as epileptic seizures but require different management.
Misdiagnosis Risks
Misdiagnosis of syncope as epilepsy or vice versa is common. Always consider both possibilities, especially when symptoms overlap.
Postural Hypotension and Specific Diagnoses
Postural hypotension requires careful evaluation. Special considerations include ruling out abdominal aortic aneurysm in older men and ectopic pregnancy in younger women.
Conclusion
Syncope is a multifaceted condition that demands careful evaluation and management in the emergency department. By understanding the underlying causes, utilizing appropriate diagnostic tools, and implementing effective management strategies, healthcare professionals can optimize patient outcomes and reduce the risk of recurrent episodes.
This guide aims to provide valuable insights into the diagnosis and management of syncope, helping healthcare providers deliver high-quality care. For further information, examples, and case studies, visit the St Emlyn's blog, where we continue to share knowledge and expertise in emergency medicine.
Remember, accurate diagnosis and timely intervention are key to managing syncope effectively. Stay vigilant, consult with senior colleagues when needed, and always prioritize patient safety.
Thank you for reading. If you have any questions or need further information, please get in touch. We look forward to continuing the conversation and improving patient care together.
Thursday Aug 07, 2014
Thursday Aug 07, 2014
Understanding High Sensitivity Troponins: A Guide for Emergency Physicians
Welcome to the St. Emlyn's podcast. I'm Ian Beardsell and I'm Rick Bodden. This is part two of our troponin special where we delve deeper into high sensitivity troponins (hs-Tn) and their significance in emergency medicine. Today, we'll explore the nuances of hs-Tn assays and how they can enhance our work in the emergency department (ED).
Introduction to High Sensitivity Troponins
High sensitivity troponins (hs-Tn) have transformed how we detect and manage myocardial infarctions (MI) in emergency settings. Unlike traditional assays, hs-Tn tests detect much lower concentrations of troponin, a protein released during myocardial injury, allowing for earlier and more accurate detection of cardiac events.
Analytical Sensitivity vs. Diagnostic Sensitivity
Understanding the difference between analytical and diagnostic sensitivity is crucial. Analytical sensitivity refers to the assay's ability to detect low concentrations of troponin, whereas diagnostic sensitivity relates to the test's performance in diagnosing acute myocardial infarctions (AMI).
Key Points on Analytical Sensitivity:
- Detection Threshold: High sensitivity troponin assays can detect troponin in over 50% of healthy individuals.
- Precision: These assays have a coefficient of variation (CV) of less than 10% at the diagnostic threshold, ensuring consistent results.
Diagnostic Sensitivity:
- Improved Detection: Studies show hs-Tn assays have a higher diagnostic sensitivity (90-92%) compared to older assays (80-85%).
- Early Rule-Outs: This makes hs-Tn particularly valuable for ruling out AMI in patients presenting with chest pain in the ED.
High Sensitivity Troponin Assays: A Closer Look
To illustrate, let's focus on the Roche troponin T high sensitivity assay:
- 99th Percentile Cutoff: 14 nanograms per liter.
- Detection Range: Can detect levels as low as 3 nanograms per liter.
- Higher Readings: It's common for hs-Tn assays to give higher readings than older assays for the same sample, which affects the diagnostic threshold.
The Balance Between Sensitivity and Specificity
While hs-Tn assays improve sensitivity, they may reduce specificity:
- More Positives: Lowering the diagnostic threshold results in more positive results, increasing diagnostic sensitivity but reducing specificity.
- Predictive Value: For example, a positive hs-Tn T result at patient arrival has a specificity around 70% and a positive predictive value of 50%.
Using High Sensitivity Troponins in the Emergency Department
Early Rule-Out Protocols: The most significant advantage of hs-Tn assays is their potential to expedite the rule-out process:
- Zero and Three-Hour Protocols: Studies suggest that hs-Tn assays can effectively rule out AMI with samples taken at 0 and 3 hours after arrival, instead of the traditional 6-hour wait.
- Efficiency: This protocol can significantly speed up patient throughput in the ED, reducing congestion and wait times.
Understanding Deltas: Delta refers to the change in troponin levels between tests:
- Absolute vs. Relative Deltas: Absolute changes (e.g., an increase of 10 nanograms per liter) are often more reliable than relative percentage changes.
- Clinical Context: It's crucial to interpret deltas in the context of the patient's overall clinical picture.
Practical Considerations for Emergency Physicians
Incidental Troponin Elevations: With increased testing at the front door, incidental findings are inevitable:
- Low Pre-Test Probability: In patients with a low pre-test probability of AMI (e.g., mechanical falls), a positive hs-Tn result often does not indicate AMI.
- Clinical Judgment: Consider repeating the test and evaluating the patient's history and clinical presentation before making a decision.
Patients with Comorbidities: Troponin levels can be elevated in patients with various comorbidities:
- Age and Chronic Conditions: Older patients and those with conditions like LV dysfunction may have higher baseline troponin levels.
- Reference Ranges: Use broader reference ranges for patients with comorbidities, as suggested by studies from Paul Collins and colleagues.
Future Directions and Guidelines
Ongoing Research: Research and guidelines on hs-Tn usage are continually evolving:
- NICE Guidelines: Recommendations on using hs-Tn in clinical practice are expected to be published, providing clearer protocols for emergency physicians.
- Early Adoption: As new evidence emerges, early adopters must balance innovation with patient safety.
Point-of-Care Testing: While hs-Tn assays currently require large analyzers, point-of-care testing remains a goal:
- Future Developments: Advances in technology may eventually make hs-Tn testing available at the bedside, further streamlining ED workflows.
Conclusion
High sensitivity troponins represent a significant advancement in the early detection and management of myocardial infarctions in the emergency department. By understanding the nuances of analytical and diagnostic sensitivity, utilizing early rule-out protocols, and interpreting results within the clinical context, emergency physicians can leverage these assays to improve patient care. As always, ongoing research and adherence to evolving guidelines will be essential in optimizing the use of hs-Tn in clinical practice.
We hope this podcast helps you better understand the complexities and advantages of high sensitivity troponins. For more insights and updates, stay tuned to the St. Emlyn's blog and feel free to reach out with your questions and experiences. Together, we can continue to advance emergency medicine for the benefit of our patients.
Wednesday Aug 06, 2014
Wednesday Aug 06, 2014

#AWESOME ALERT - CLIFF REID WILL BE THERE - YOU HAVE TO BE TOO!!!!
I'll be there with many others from St.Emlyn's so if you see me say hi.
You can see the program here
vb
S
Sunday Jul 27, 2014
Monday Jul 21, 2014
Monday Jul 21, 2014
Starting Your Career in Emergency Medicine: Key Insights from St. Emlyn’s
Welcome to the world of emergency medicine! At St. Emlyn’s, we understand the challenges and excitement that come with starting your career in this fast-paced field. Whether you’re a new doctor stepping into the emergency department (ED) for the first time or a medical student gearing up for your rotation, we’ve got you covered. This post delves into the nuances of emergency medicine, sharing valuable insights from seasoned professionals, Iain Beardsell and Simon Carley, to help you navigate your journey effectively.
Understanding the Unique Nature of Emergency Medicine
Emergency medicine is distinct from other medical disciplines. Unlike the traditional approach taught in medical school, which involves extensive histories and comprehensive examinations, emergency medicine requires quick, focused thinking and decisive action. The goal is to identify and address life-threatening conditions promptly.
Time-Pressured Environment
In the ED, time is of the essence. Patients arrive needing immediate care, and as an emergency physician, you won’t have the luxury of lengthy deliberations. Your patients want answers quickly, and this urgency shapes the way you practice. You’ll learn to focus on the presenting problem and drill down into the most critical aspects of their condition.
Different Thinking Model
The thinking model in emergency medicine is primarily hyperthetico-deductive reasoning. This means you’ll form hypotheses based on initial information and then test these hypotheses through targeted questions and examinations. For instance, if a 55-year-old man presents with central crushing chest pain radiating down his left arm, your first thought should be an acute myocardial infarction (AMI).
Prioritizing Life-Threatening Conditions
One of the fundamental differences in emergency medicine is the approach to diagnosing and treating conditions. Instead of trying to confirm what a patient has, you’ll focus on ruling out what they don’t have, especially the most life-threatening possibilities. For example, with chest pain, you’ll consider AMI, pulmonary embolism (PE), and aortic dissection as top priorities.
The 10% Rule
Interestingly, about 10% of patients presenting with symptoms like chest pain or headache have significant pathology. Your job is to identify this 10% while efficiently managing the remaining 90%. This approach ensures that you don’t miss critical diagnoses while not overburdening yourself with unnecessary details.
Practical Steps for Your First Shift
As you prepare for your first shift in the ED, here are some practical steps and philosophies to keep in mind:
Resuscitation First
Your primary goal is to identify if a patient needs resuscitation. Are they critically unwell? Do they require urgent interventions to save their life? This is your top priority.
Pain Management
After ensuring resuscitation, your next focus should be pain management. A pain-free emergency department is a goal to strive for. Administer analgesia as needed to ensure patient comfort, even before completing a full history or examination.
Rule Out Life-Threatening Conditions
When a patient presents with a complaint, think about the worst-case scenarios related to their symptoms and aim to rule these out. For example, with chest pain, consider whether the patient might have an AMI, PE, or aortic dissection.
Focused History and Examination
Conduct a focused history and examination to gather information pertinent to the presenting complaint. Avoid getting bogged down with irrelevant past medical history unless it directly impacts the current situation.
Implementing the Four Big Hitters
Simon and Iain emphasize the importance of considering four key interventions for every patient:
- Oxygen: Determine if the patient needs oxygen or airway support.
- Analgesia: Ensure adequate pain relief is provided.
- Fluids: Assess if the patient would benefit from intravenous fluids.
- Antibiotics: Consider if antibiotics are necessary for their condition.
Learning and Growing in the ED
The ED is a dynamic learning environment. Here’s how you can maximize your growth and effectiveness:
Ask Questions
Don’t hesitate to ask questions. No question is too silly. Engaging with senior colleagues and seeking their advice will enhance your learning and patient care skills.
Continuous Learning
Emergency medicine is a field where continuous learning is crucial. Keep up with the latest practices, guidelines, and innovations. Attend workshops, conferences, and training sessions to stay updated.
Collaborative Approach
Remember that emergency medicine is a team effort. Collaborate with nurses, paramedics, and other healthcare professionals. Effective communication and teamwork are essential for providing the best patient care.
Reflect and Improve
After each shift, take time to reflect on your experiences. Identify what went well and areas for improvement. This self-assessment will help you grow as a clinician and enhance your skills over time.
The Importance of Confidence and Competence
Confidence in your abilities is vital, but it must be balanced with competence. Strive to be competent in your practice, and your confidence will naturally follow. Be aware of the balance between these two aspects to avoid the pitfalls of overconfidence.
Unconscious Incompetence
One of the dangers in any medical field is unconscious incompetence—being unaware of what you don’t know. Stay humble, keep learning, and seek feedback from peers and seniors to continuously improve your competence.
Embracing the ED Culture
The culture in the ED is unique. It’s a place where decisive actions and quick thinking are valued. Embrace this culture and the opportunities it presents for hands-on learning and making a real difference in patients’ lives.
A Little Less Conversation, A Little More Action
In the ED, the Elvis philosophy—“a little less conversation, a little more action”—applies. Focus on doing what’s necessary for the patient rather than getting caught up in lengthy discussions. This action-oriented approach is crucial for effective emergency care.
Conclusion: Your Journey Ahead
Starting your career in emergency medicine is both exciting and challenging. At St. Emlyn’s, we believe in providing you with the tools, knowledge, and support you need to succeed. Remember the key principles: prioritize life-threatening conditions, focus on critical interventions, continuously learn and ask questions, and embrace the dynamic culture of the ED.
We love our jobs and hope that you, too, will find the same passion and fulfillment in your career. Good luck, enjoy the journey, and know that we’ll be with you every step of the way through this podcast and our wider St. Emlyn’s community.
Welcome to the world of emergency medicine. Let’s make a difference together!